Download
1 / 29
290 likes | 529 Views
Chronic Obstructive Pulmonary Diseases (COPD) Chronic Airflow Limitation (CAL). Emphysema . Loss of lung elasticity Hyperinflation of the lung Formation of Bullae Small airway collapse and air trapping. Classifying Emphysema.

E N D
Chronic Obstructive Pulmonary Diseases (COPD) Chronic Airflow Limitation (CAL)
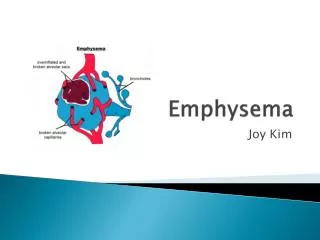
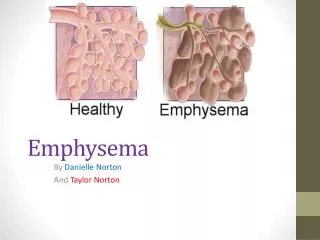
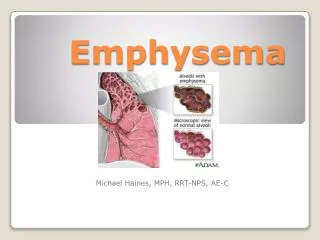
Emphysema • Loss of lung elasticity • Hyperinflation of the lung • Formation of Bullae • Small airway collapse and air trapping
Classifying Emphysema • Panlobular • Centrolobular
Clinical Manifestations • Progressive dyspnea on exertion • Prolonged expiratory phase & tachypnea • Increased work of breathing • Anorexia, weight loss • Barrel Chest • Flattened diaphragm
Clinical Manifestations (cont) • Formation of blebs and bullae • Hyperresonance • Polycythemia (pink puffer) • Chronic hypoxia • Pneumothorax • Hypercapnic to hypoxic drive • Chronic respiratory acidosis (end stage)
Pulmonary Function Tests • Increased • residual volume • total lung capacity • Decreased • Forced vital capacity • FEV1
Chronic Bronchitis • Excessive production of mucus in the bronchi • Productive cough • Persists 3 months of the year for 2 consecutive years
Pathologic Changes • Chronic inflammation • Hypertrophy and hyperplasia of the mucus glands • Increased susceptibility to infection • V/Q changes
Presentation • May have same symptoms as emphysema • Frequent respiratory infections • Cyanosis • Cor pulmonale • Polycythemia
Asthma • Not always listed as one of the diseases of COPD/CAL • Asthma is usually a reversible process • Involves periodic episodes
Asthma Classifications • Extrinsic (Allergic) • Antigen/antibody response • Childhood • Intrinsic (Endogenous) • History recurrent RTI • adulthood
Pathologic Changes • Hypersensitivity response • Bronchoconstriction • May become chronic with irreversible changes
Presentation • Bronchospasm • Increased mucus secretion • Dyspnea • Wheezing • Cough
Consequences of CAL • ABG’s • Initially normal ABG followed by decreased PaO2 and O2 saturation • Increased PaCO2 with an increase in HCO3 to compensate • Compensated Respiratory Acidosis and Hypoxemia
Polycythemia • Related to decreased PaO2 • What is the mechanism?
Pulmonary Function Tests • What do you expect? TLC increased FEV1 decreased
Cor Pulmonale COPD/CAL Pulmonary Vascular Bed Pulm Hypertension Hypoxemia RV Failure Polycythemia LV Failure
Collaborative Management of CAL • Medical management • Maximize oxygenation, ventilation and perfusion • Surgical management • Bullectomy • Lung volume reduction surgery
Drug Therapy • Bronchodilators • Sympathomimetics • Methylxanthines • Anticholinergics • Steroids • Mast Cell Stabilizers • Leukotriene Antagonists • Expectorants • Antibiotics
Nursing Diagnoses • Impaired gas exchange • Ineffective airway clearance • Activity intolerance • Anxiety • Altered nutrition: less than body requirements
Nursing Interventions • Maintain a patent airway • Safely administer oxygen • Use oxygen delivery systems appropriately • Accurately assess the patient’s breathing • Use positioning to improve oxygenation
Teach the Patient: • Abdominal & Pursed lip breathing • Controlled coughing • Conservation of energy • Prevent secondary infection • Insure hydration • Nutrition • Therapeutic communication/relaxation