Download
1 / 16
260 likes | 861 Views
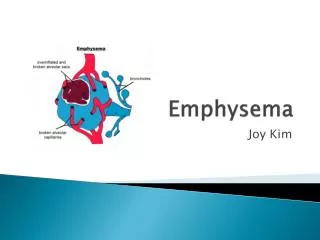
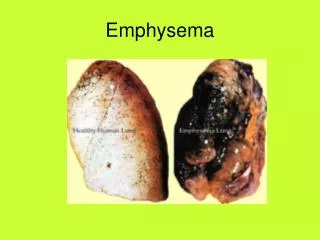
Tanya Holubiak MD4 # 1075. EMPHYSEMA. “Emphysema is a condition of the lung characterized by abnormal permanent enlargement of the airspaces distal to the terminal bronchiole, accompanied by destruction of their walls and without obvious fibrosis” †. Definition. What is Emphysema?.

E N D
Tanya Holubiak MD4 # 1075 EMPHYSEMA
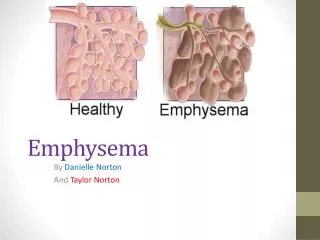
“Emphysema is a condition of the lung characterized by abnormal permanent enlargement of the airspaces distal to the terminal bronchiole, accompanied by destruction of their walls and without obvious fibrosis” † Definition
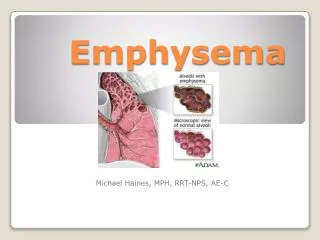
What is Emphysema? • General Considerations: • COPD • Permanent enlargement & destruction of airspaces • Loss of lung elasticity
4 Major Types • CENTRILOBULAR (centriacinar) • PANACINAR • PARASEPTAL • IRREGULAR • Other Types • Compensatory Hyperinflation • Obstructive Overinflation • Bullous Emphysema • Interstitial Emphysema
4 Major Types CENTRILOBULAR PANACINAR Enlargement is uniform from the respiratory bronchioles to the alveoli Tends to occur in the lower lung field & anterior margins, most severe form at the bases of the lung Cause is associated with Alpha 1-Antitrypsin deficiency Grossly increased size of the alveolar space & monotonous appearance ‡ • Enlargement of the centrilobular airspaces • Damage affects mainly the proximal & central respiratory bronchioles • Distal Alveoli spared • Commonly distributed in the upper lobe • Development believed to be correlated cigarette smoking, dust inhalation, & residents of smog filled cities‡ • Characteristic gross appearance is anthracosis in a patchy fashion
4 Major Types (cont’d) PARASEPTAL IRREGULAR Acinus is irregularly involved Almost always is associated with scarring • Enlargement of the airspaces at the distal acinar • Lesions mostly along the dorsal surface of the upper lung† • Occurs along scarring & atelectasis • Often associated with fibrosis & may coexist w/ other emphysema • Responsible for spontatneous pneumothorax in young males
PATHOPHYSIOLOGY Major Physiologic Changes in the Lungs³ Physiologic Effects vary & depend on the severity of disease³ Relative degree of Bronchiolar obstruction vs. Lung Parenchymal destruction Irregularities include: Increases in Airway Resistance Decreases in Diffusing Capacity Massively Abnormal Ventilation-Perfusion ratios Pulmonary Hypertension • Chronic Infection from inhalation of smoke or other irritants that aggravate bronchi & bronchioles • Chronic Obstruction of many smaller airways • Entrapment of Air in the Aveoli & overstretching them
PATHOGENESIS Protease-Antiprotease Theory • Hypothesis to explain the damage of alveolar wall • Imbalances of protease-antiprotease & oxidant-antioxidant have additive effect on tissue damage • Excessive Protease + Less Anti-protease • Cigarette smoking • Contains Oxidants • Cause PMNs to release free oxy radicals • Inhibit α1-AT • Neutrophil elastase release • Particles @ bifurcation of respiratory bronchioles • Engulfed by macrophages • release elastase & metalloproteinases • Released elastase can digest α1AT • Cause lung tissue damage
CLINICAL FINDINGS • Dyspnea • Weight Loss • Variable Coughing & Expectoration • Wheezing • Barrel-chested • Prolonged Expiration • Hunched-over sitting position • Breathing through pursed lips • Severe Emphysema • Cough is slight • Severe Overdistention • Diffusion Capacity is low • Blood gas fairly normal @ rest • “Pink Puffers” • Overventilation • Well oxygenated
CLINICAL FINDINGS (cont’d) • Death in most COPD patients from: • Respiratory Acidosis & Coma • Right-sided Heart Failure • Massive Collapse of the Lungs
DIAGNOSIS • Spirometry • High Resolution Computed Tomography (HRCT)
HRCT Normal Lung Moderate Centrilobular Panacinar HRCT of the normal lung. The pulmonary artery supplies 2 secondary lobules, and arrows indicate branching on the intralobular airways On HRCT, a “wall” structure is observed at the periphery of the emphysema, composed of compressed lung tissue and perilobularvessels. On HRCT, diffuse low attenuation changes are aboservedthrought out the lung field.
MANAGEMENT/TREATMENT Usual Options for Tx: In Selected Patients Lung Volume Reduction Surgery Lung Transplantation • Bronchodilators • Steroids • Bullectomy
CASE STUDY⁴ 57 year-old-man with severe, disabling end-stage emphysema was randomly assigned to a surgery group. Before surgery, the patient was able to walk only 100 to 200 yd (91-183 m) on level ground because of dyspnea & not able to perform the activities of daily living. Preoperative axial CT showed severe, heterogenous emphysema that predominantly affected the upper lobes. Color-enhance, 3D, volume-rendered imaging was used. This method showed, in this case, a marked predilection of the emphysema for the upper lobes.
CASE STUDY cont’d • Patient underwent bilateral video-assisted thoracoscopic surgery, with resection of the majority of the right upper lobe. • 1 year post-op: Patient was able to was a little more than 1 mile (1.6 km)
REFERENCES † Abbas, Abdul K. et. al. Robbins and Cotran: Pathologic Basis of Disease 7th Edition. Philadelphia, PA: Elsevier Inc., 2005. ‡ Takahashi, Masashi et. al. “Imaging of pulmonary emphysema: A pictorial review.” 2008. International Journal of COPD. Ed. Dove Press Vol. 3(2). 193-204. ³ Guyton, Arthur C. and Hall, John E. Textbook of Medical Physiology 11th Edition. Philadephia, PA : Elsevier Inc., 2006. ⁴Hunsaker, Andetta R. and Reilly, John J. “Centrilobular Emphysema with Predominantly Upper-Lobe Involvement.” 2003 New England Journal of Medicine. Massachusetts Medical Society. Vol. 348. 2091