Download
1 / 28
340 likes | 934 Views
Carotid Body Tumour. Dr. Maha Al Marashi. KM. 34 Female. Elective admission for Right Carotid body tumour excision Had been referred initially to the vascular service with bilateral carotid body tumours Incidental finding with no local pressure symptoms or systemic effects. KM. 34 Female.

E N D
Carotid Body Tumour Dr. Maha Al Marashi
KM. 34 Female • Elective admission for Right Carotid body tumour excision • Had been referred initially to the vascular service with bilateral carotid body tumours • Incidental finding with no local pressure symptoms or systemic effects
KM. 34 Female • BGHx: • Left carotid body tumour embolizaion • Appendectomy as a child • Tonsillectomy as a child
KM. 34 Female • Medications: • Nil • Allergies: • Nil
KM. 34 Female • Family Hx: • Grandfather – Carotid body tumour • Brother – Carotid body tumour bilaterally
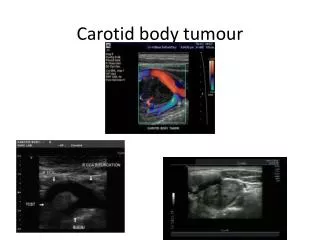
KM. 34 Female • Ultrasound scan neck • Evidence of bilateral carotid body tumours of the carotid bifurcation consistent with carotid body tumours. • Thyroid gland is normal. • No other abnormalities.
KM. 34 Female • Duplex scan of carotids • Bilateral masses in the region of the carotid body at the bifurcation of the internal and external carotids. • Right is smaller and more vascular. • Left encases vasculature.
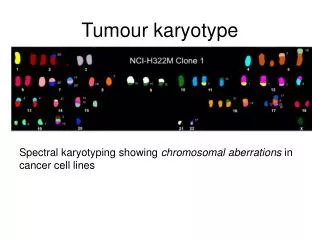
KM. 34 Female • Genetic screening:
KM. 34 Female • Right carotid body tumour excision
KM. 34 Female • Histology:
KM. 34 Female • Discharged home day 2 post op with no complications • Simple analgesia and aspirin • For OPD follow up in 4 weeks.
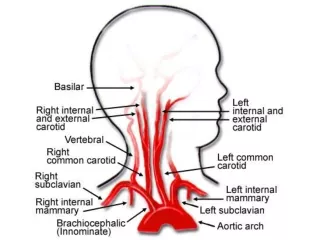
Anatomy • Bifurcation of the common carotid artery • Right side coming of the brachiocephalic artery • Left side from arch of aorta
Anatomy • Thyroid gland • Trachea • Brachiocephalic artery • Common carotid artery • Internal jugular vein • Superior vena cava
Embryology • Derived from: • Mesodermal elements of the third branchial arch • Neural elements originating from the neural crest ectoderm • Neural crests differentiate into forerunners of paraganglionic cells • Paragangangliomas
Physiology • Chemoreceptors located in the bifurcation of the common carotid artery • Monitor changes in the oxygen and CO2 content and pH of the blood and rely that sensory information to the hypothalmus and brain stem to help them control cardiovascular and respiratory functions • Other cells in the carotid body respond to blood temperature and to certain chemicals, e.g., nicotine and cyanide. • Has extremely high blood flow and oxygen consumption
Histology • Resemble the normal architecture of the carotid body • Highly vascular • Zellballen (cell nests) • “Sustentacular” cell • Epithelioid cell • Cytochemical techniques have demonstrated: • Adrenaline • Noradrenaline • Serotonin
Classification • Chromaffin • Capable of producing catecholamines • Non-chromaffin • Initially, Carotid body tumours were thought to be non-chromaffin paragangliomas • ≤5% of carotid body tumours are endocrinologically active • May be part of the neurocristopathies e.g. MEN 1 & 2 • Secondary tumours are common, including phaeochromocytomas
Pathology • Only known pathology is neoplasia • Most common of the non-chromaffin paragangliomas • Shamblin et al described the following anatomic groups: • Group 1: small tumours, minimally attached. Surgical excision not difficult • Group 2: larger, moderate attachments. Can be resected, but many require temporary intra-luminal carotid shunt • Group 3: very large, encase carotid arteries. Often require arterial resection and grafting
Incidence • Sporadic • More common • 5% incidence of bilateral tumours • Familial • Autosomal dominant • 32% incidence of bilateral tumours • Men:Women = 1:1 • Screening of family members recommended • Age • Range between 20-80 • Most apparent in 5th decade
Biologic behaviour • Malignant potential • Cannot be predicted by histological markers • Made by presence of lymph nodes or metastases • Metastatic spread • In region of lymph nodes • Kidney, thyroid, pancreas, cerebellum, lungs, bones, brachial plexus, abdomen and breast • Rate approximately 5% • Predictors • Severity of symptoms • Size at time of diagnosis
History • Painless swelling in neck at the angle of the mandible • Non-specific • Neck or ear pain • Local tenderness • Hoarseness • Dysphagia • Tinnitus • Occasionally • Cranial nerve dysfunction • Rarely • Lateralizing central neurological signs or symptoms • Neurosecretory • Dizziness • Flushing • Palpitations • Tachycardia and arrhythmias • Headache and photophobia • Diaphoresis
Examination • Neck mass below the angle of the mandible • Laterally mobile but vertically fixed • Non-tender, rubbery, firm and non-compressible • Often pulsatile • Bruit • Abnormalities caused by vagal or hypoglossal nerve impingement • Horner’s syndrome (rare) • Palpate opposite side
Differential diagnosis • Lymphoma • Metastatic tumours • Carotid artery aneurysm • Thyroid lesions • Submandibular salivary gland tumours • Branchial cleft cysts
Investigations • Duplex scan with colour flow imaging • Documents the highly vascularised mass in the area of carotid bifurcation • Tumour dimensions • Co-existent carotid occlusive disease • Angiography • Gold standard • Identifies collaterals, concurrent atherosclerosis and multicentric disease • Dynamic or rapid sequencing CT • Differentiates between aneurysm and neoplasm • Size and extent • MRI • Demonstrates relationship of tumour to adjacent structures • Differentiate from other soft tissue lesions at base of skull • Size and extent
Management • Mainstay is complete surgical excision due to: • ≥5% incidence of metastases • Unrelenting growth of unresected tumours • Early excision decreases incidence of cranial nerve and carotid artery damage • Most are in Shamblin’s group 2 or 3 at time of clinical presentation • Radiation for local control of residual or recurrent disease • Chemotherapy has no role • Pre-operative embolization • Pros: Decrease vascularity and improve safety • Cons: thrombosis of ICA or cerebral embolization
Prognosis • Carotid body tumours are slow growing and exhibit benign characteristics • Can survive for long periods without surgical intervention • Death due to asphyxia and intra-cranial extension; Martin et al noticed death rate of approximately 8% in untreated patients • Even after prolonged disease-free intervals, local recurrence following surgical resection described