Download
1 / 23
230 likes | 399 Views
Carotid Pathology II. Fibromuscular Dysplasia. Characterized by fibro tissue proliferation. Arterial involvement segmental up to several cm. ICA most common of cervical vessels 85%. May result in carotid dissection & or thrombotic embolic. Fibromuscular Dysplasia. Mid-Distal ICA.

E N D
Fibromuscular Dysplasia • Characterized by fibro tissue proliferation. • Arterial involvement segmental up to several cm. • ICA most common of cervical vessels 85%. • May result in carotid dissection & or thrombotic embolic.
Fibromuscular Dysplasia Mid-Distal ICA “String of Beads”
Fibromuscular Dysplasia Alternating Zones of Narrowing by Spectral Normal ICA Waveform
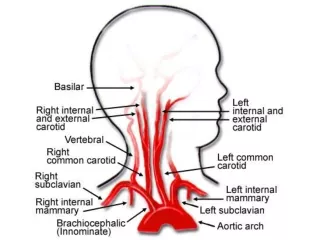
Subclavian Steal Phenomenon • Occurs with a high-grade stenosis or occlusion of the proximal subclavian or innominate arteries. • Diversion of blood from the high-pressure vertebrobasilar circulation to the low-pressure upper extremity circulation via “Retrograde” vertebral artery flow. • Brachial systolic pressure > 15-20 mm Hg indicates obstruction
Subclavian Steal Phenomenon 85% 15%
Subclavian Steal Phenomenon Incomplete Complete Bunny/Pre-steal Tardus-Parvus
Subclavian Steal Phenomenon Right Vertebral
Subclavian Steal Phenomenon Left Vertebral
Subclavian Steal Phenomenon Right Subclavian
Subclavian Steal Phenomenon Incomplete to Complete Steal Cuff Induced Hyperemia Incomplete Steal
Carotid Endarterectomy • Diseased intima “shelled” out & artery wall closed/sutured • Vein patch or Synthetic material (polytetrafluoroethylene) used to enlarge site of stenotic narrowing • Duplex sonography to confirm patency, presence of flaps, & stenosis due to neointimal hyperplasia
Follow-Up Carotid Endarterectomy • 3, 6, 12 Month follow-up exams • Postendarterectomy flow disturbances: • spectral broadening - rough subintimal layer, • stenosis/occlusion caused • by intimal flap • retained plaque • neointimal hyperplasia, • ICA often exhibits an “Externalized” waveform
Follow-Up Carotid Endarterectomy • 2 years post surgery when most (70%) of re-stenosis occur. • Re-stenosis within the first 3 years results from progression of neointimal hyperplasia.
Follow-Up Carotid Endarterectomy Normal Turbulence
Follow-Up Carotid Endarterectomy Graft ICA
Follow-Up Carotid Endarterectomy Neointimal Hyperplasia Stenosis