Download
1 / 19
190 likes | 354 Views
DMI 56 ~Ch. 7 Cardiovascular System. Marilyn Rose RT, RDMS. Physiology of Cardiovascular System Congenital Heart Disease Acquired Vascular Disease Valvular Disease Pericardial effusion Venous Disease. outline. Function = maintain adequate supply of blood to all the tissues of the body

E N D
DMI 56 ~Ch. 7Cardiovascular System Marilyn Rose RT, RDMS
Physiology of Cardiovascular System • Congenital Heart Disease • Acquired Vascular Disease • Valvular Disease • Pericardial effusion • Venous Disease outline
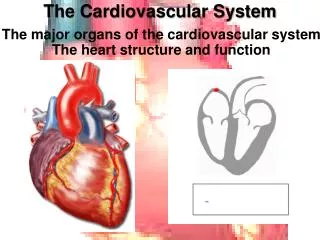
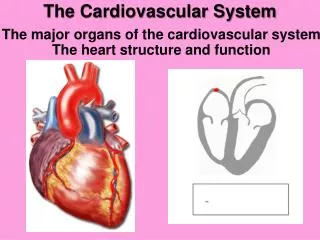
Function= maintain adequate supply of blood to all the tissues of the body • Autonomic nervous system controlled contractions • Vagus nerve slows heart rate with acetylcholine • Sympathetic nervous system stimulates the release of epinephrine to accelerate the heart rate/ > force • 4 chambers- striated muscle • walls lined with endocardium- continuous with blood vessel lining • Between each atria/ ventricle are atrioventricular valves- • permit blood to flow in one direction Physiology
Mitral valve- bicuspid- left • Tricuspid valve- right • Semilunar- separate great vessels and ventricles • Pulmonary valve- right ventricle and pulmonary artery • Aortic valve- left ventricle and aorta • Do2 blood returned by SVC to right atrium • O2 blood- pulmonary veins to left atrium • Systole- contraction • Diastole- relaxation • Normal cardiac impulse to contract arises • SA node- pacemaker (intrinsic) • right atrial wall at the opening of the SVC Physiology
Left to Right Shunts • Most common congenital lesion • Permit mixing systemic and pulmonary circulation • Lungs become overloaded • Enlargement of chambers- depending on location • Can be complicated by pulmonary hypertension • A. atrial septal defect (most common) • Lack of closure of the foramen ovale after birth/ or premature • Radiographic- > right, ventricle/ atrium and pulmonary outflow tract • B. ventricular septal defect • > pulmonary blood flow and > pulmonary venous return • Diastolic overloading- > left atrium and > left ventricle • C. patent ductus arteriosis • Intrauterine- shunts blood from pulmonary artery to the systemic circulation • > pulmonary blood flow > blood returned to Lt atrium/ ventricle • Radiograpic- > left atrium/ ventricle and pulmonary arteries Congenital Heart Disease-1
Tetralogy of Fallot • Most common cause of cyanotic congenital heart disease • Consists of (4-tetra) abnormalities: • 1. high VSD • 2. pulmonary stenosis • > RV pressure, • Narrow pulm valve- inadequate blood supply tolungs • 3. overriding AO above VSD- right to left shunting • doO2 blood into left vent and systemic circulation • 4. right ventricular hypertrophy (enlargement) • Radiographic- enlargement of RV causes upward/ lat displacement of the heart apex • ¼ of patients- AO on right side CHD- 2
Coarctation of the Aorta • Narrowing, or constriction of the aorta • Beyond branching blood vessels to the head and arms • Higher- blood supply and pressure to upper extremities • Normal BP in arms • Decreased blood flow to abdomen legs • Low BP in legs • Most frequent cause for HTN in children • Collateral circulation develops • Radiographic • Rib notching (post 4th to 8th) from pressure erosion of dilated intercostal collateral vessels • Two bulges in the aortic knob- 3sign on xray • ECHO is primarily used to evaluate the stenosis and severity of blood flow compromised CHD-3
Coronary Artery Disease • Narrowing causes O2 deprivation of myocardium • Ischemic heart disease • Atherosclerosis risk factors- • HTN, obesity, smoking, high cholesterol diet, lack of exercise • Angina pectoris- temporary O2 insufficiency • Severe chest pain radiates to neck, jaw, left arm • Attacks happen with > O2 demand by myocardium- after exercise, a heavy meal, emotional stress, severe cold • Nitroglycerine- > venous dilation and >02 to myocardium • MI- occlusion of a coronary artery- death of muscle cells • The greater the area affected- poorer the prognosis • A favorable prognosis- collateral circulation • Radiographic: • Radionuclide thallium perfusion is the major noninvasive study (nuc med) • SPECT – new technique for necrosis • Plain CXR are normal • IVUS most precise anatomic information Acquired Vascular Disease-1
CHF • Inability of heart to propel blood rate and volume to provide an adequate supply to tissue • Causes- intrinsic cardiac abnormality (insuf or defective cardiac filling, impaired contractions) HTN, any obstructive process that abnormally > the peripheral resistance to blood flow • Radiographic • Left sided heart failure produces a classic appearance of cardiac enlargement and redistribution of pulmonary venous blood flow, interstitial edema, alveolar edema, pleural effusion • Acute left ventricular failure from CAD • May be severe pulmonary congestion/ edema with very little cardiac enlargement • Change in technique for increased pleural fluid • Lt sided heart failure- CAD, valvular, HTN • Rt sided heart failure • dilation of right atria/ ventricle • Increased pressure cause dilation of SVC, edema of lower extremities • Pulm vascular stenosis, emphysema, pulm HTN- resulting from pulm emboli • Cardiomegaly- evaluate from PA chest- cardiothoracic ration- >50% • (label well) • Echocardiography is modality of choice Acquired-2
Pulmonary Edema • Abnormal accumulation of fluid in extravascular pulm tissue • Common cause is elevation of pulmonary venous pressure • Other causes: pressure from LT heart failure, or pulm venous obstruction, lymphatic blockage or metastatic disease with involvement of mediastinal lymph nodes, uremia, narcotic overdose, exposure to noxious fumes, excessive O2, high altitude, fat embolism, adult respiratory distress syndrome, neurologic abn • Radiographic • Earliest stage- transudation of fluids into interstitial spaces of lungs • > pulm venous pressure first appears as redistribution of blood flow from lower to upper lung zones • Loss of normal definition of pulm vascular markings- perihilar haze • Alveolar edema appears as irregular, poorly defined patchy densities scattered thru the lungs • Classic finding- “butterfly pattern”- bilat symmetric fan shaped prominent in central portion of lungs • Pleural effusions usually occurs on the right side • Lateral decubitus Acquired-3
Hypertension (HTN) • High blood pressure • Leading cause of strokes and CHF • Blood pressure is a function of cardiac output and total peripheral resistance (condition of blood vessel walls throughout the body) • Peripheral resistance/ cardic output can vary with sitting, standing, quiet/ excited- yet systemic pressure remains constant in a healthy person • Systolic- highest in peripheral arteries- @ lt vent contraction • Diastolic- pressure in peripheral arteries as lt vent relaxes- fills • High blood pressure >140/ 90 (additional 10 systolic every decade over 40) • Benign- HTN of gradual onset and prolonged for many years • Malignant- abrupt onset, rapid cousrs and renal failure or cerebral hemorrhage. • 6% secondary HTN • Radiographic • Arteriography is most accurate for renovascular lesions • Renal artery narrowing from atherosclerosis • CT for renal artery stenosis or FMD…however US has found it too. • FMD- sting of beads, women, bilateral Acquired- 4
Aneurysm • Localized dilation of an artery • Most commonly involves the aorta • Below renal arteries • Saccular one side of the arterial wall • Fusiform- bulging of entire circumference of vessel • Represents a weakness in wall by • atherosclerosis, syphilis or cong defect- Marfan’s • Rupture and massive hemorrhage • Radiographic: • Ultrasound is modality of choice- AAA • Diameter >3 cm • CTA and MRA location and extent- replace angio • CTA retroperitoneal or rupture of an aneurysm Acquired -5
Traumatic rupture of the aorta • Potentially fatal from closed chest trauma • Rapid deceleration, blast, compression • Aortic tear just distal to left subclavian artery • Radiographic • Hemorrhage into the mediastinum= widening of silhouette • Rib or sternal fx • CT best modality- laceration or ao rupture Acquired-6
Dissection of the aorta • Potentially life threatening • Disruption of the intima ( inner layer) allows blood to enter the wall of the aorta and separate the layers • Aorta is divided into a true and false lumen • The false lumen can form an aneurysm • Occur in patients with arterial hypertension, trauma or Marfan’s • Sudden sharp pain with death days later with rupture of aneurysm into the chest or abdominal cavity • Type 1- 2/3 continue into descending AO • Type 2- limited to ascending AO • Type 3- begins in thoracic and extends prox and dist to origial site • Radiographic- • CT is modality of choice- detect intimal flap Acquired-7
Atherosclerosis • Thickening, hardening and loss of elasticity in the arterial wall • Major cause of valvular disease of the extremities is atherosclerosis • plaque develop • Progressive narrowing- to complete occlusion • SFA above knee • Coronary and cerebral arteries • Myocardial infarction or stroke • Radiographic • Ca++ and appear on plain radiographs as irregular densities along the artery wall • Doppler US is preferred as a non invasive evaluation for the progression of the disease • Assess luminal stenosis Acquired-8
Thrombosis/ Embolism • Blood clotting mechanism is a major protective device of the body for escape of blood from a vessel ( hemorrhage) • When it occurs in intact vessels an intravascular clot is called a thrombus • Three factors contribute: • 1. Slow flowing blood • veins or areas of stasis- inactive or immobilized (post surgery) • 2. Change in the wall of blood vessels- from smooth to rough • 3. Change in blood itself- low level of O2- >RBC- more viscous • Once thrombus forms will • 1. contract • 2. continue to enlarge- convert to fibrous tissue • Production of a embolism- detaches from wall and enters the blood stream- lodges in small blood vessels- usually the lung • Radiographic • Most common in the lower extremities Acquired-9
Rheumatic Heart • Rheumatic fever- autoimmune from reaction of patients antibodies against strep infection- less common due to antibiotics • Damage to valves of the heart- mitral and aortic • Deposits of platelets and fibrin make vegetation- stenotic valves causing insufficiency • Mitral stenosis/ insufficiency • Complication of rheumatic dz/ rupture of chordae tendinae • Aortic stenosis • Rheumatic hrtdz or congenital valvular deformity- bicuspid • Left ventricle hypertrophy Valvular Dz
Pericardial effusion is the accumulation of fluid within the pericardial space surrounding the heart • From bacteria, virus, neoplasm • Rapid accumulation- interfere with cardiac function • Slow- allows pericardium to expand • Echo is most effective Pericardial effusion
Deep vein thrombosis • DVT involves the lower extremities • Major source of potentially fatal pulmonary embolism • Trauma, bacterial infection, prolonged bed rest, oral contraceptives • May be early sign of unsuspected malignancy of pancreas, lung or GI • Radiographic • Doppler US- 95% accurate • Compression and augmentation • Filling defect with color doppler Venous Dz