Download
1 / 15
150 likes | 350 Views
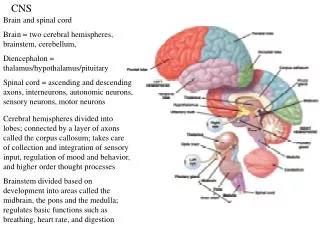
Jeanette Ribton Oncology CNS . Chemotherapy Out of Hours Triage: Neutopenic Fever. St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09. Project No: 26 08/09 Produced by: J Anders C-GARRD Presented: September 2008 . Why we needed to change: Case Study.

E N D
Jeanette Ribton Oncology CNS Chemotherapy Out of Hours Triage: Neutopenic Fever St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09 Project No: 26 08/09 Produced by: J Anders C-GARRD Presented: September 2008
Why we needed to change: Case Study • Lung cancer – early SCLC • Potential remission 2 yrs + with treatment • Co-morbidity – Eaton Lambert (poor mobility) • Pt given 1 cycle – discharged home • On day 8 - diarrhoea, unwell, low grade pyrexia • Attended A&E 1am - Hypotensive, Neuts 0.1, fluids administered • Transferred to a ward • Transferred on again Antibiotics given at 1 pm • Patient died at 4 pm St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09
Background • Snap shot Audit (randomly selected patients 2005-07) • Pre-pathway audit identified: • Lack of inpatient beds • Lack of awareness of care pathways in A&E • Poor communication across inpatient ward and A&E • Absence of IV antibiotics (for Neut sepsis) in A&E • Negative impact of 4 hour targets with patients moved off A&E prior to treatment • Delays in first antibiotic that exceeded 12 hours in several cases • Delayed first antibiotic on cancer day unit due to lack of medical staff St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09
Background A snap shot analysis illustrated: • Time for a patient to see a Doctor ranged from; 53mins to 3hrs 8mins from arrival at A&E • Time to first administration of antibiotics ranged from; 3hrs 5mins to 12hrs from arrival at A&E St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09
Initial actions • The process involved multi-professional collaboration through • the oncology and A&E departments to enable: • The development of an alert card • The development of an A&E triage neutropenic sepsis pathway (integrated into the standard A&E generic pathway) • Immediate Full Blood Count • First antibiotic administration in A&E • Broad spectrum antibiotics stored on A&E • Educational meetings to inform staff/patients of the process • Pilot period to ensure that it is patient friendly and usable • Nurse led admission (working hours) • Development of Patient Group Directives • Admission pathway St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09
Refer to unwell adult flowchart YELLOW ORANGE Inform senior Dr and coordinator At presentation If TEMP > 37.5 BP, Pulse, Resp rate IMMEDIATE FBC, U&E If clinical signs of shock – pallor, mottled skin, tachycardia, hypotension, ^resp rate, altered GCS Pts on steroids /analgesics or dehydrated may not present with pyrexia but may still have infection If Neutrophil count < 1.0 Commence IV antibiotics ASAP before pt leaves A&E Commence IV antibiotics IMMEDIATELY Without FBC result Tazocin & Gentamicin (4.5g tds) (5mg/kg od) Gentamicin should not be given with cisplatin chemotherapy If allergic to penicillin (skin rash) Gentamicin & Ceftazidime (5mg/kg od) (2g tds) If allergic reaction is anaphylaxis, uticaria, or rash immediately after penicillin must discuss management with microbiologist If Neutrophil count > 1.0: If no focus of bacterial infection and no signs of systemic infection oral antibiotics may be considered Requires medical admission Prioritize for G5
Background • Post pathway results: • The preliminary results are favorable after the implementation of the alert card and neutropenic pathway • Shortened time to first medical assessment; Ranged from 11mins to 1 hr 9mins • Reduced time to first antibiotic administration; Ranged from 1hr 38mins to 2hrs 22mins • First antibiotic dose administered in A&E • Greater understanding and enthusiasm of A&E staff St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09
Further audit St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09 • To undertake a more robust audit • To determine if the initial changes following the snap shot audit have improved the patient journey • To identify any problems with the new pathway • To measure patient outcomes • High Risk/Low risk using the MASCC tool • Length of stay • Length of antibiotics • Mortality • To identify future potential changes to improve the inpatient experience
Determining high/low risk groups Risk determined through MASCC score (Multinational Association of Supportive Care in Cancer) Score > 21 = low risk Score < 21 = high risk
Methodology Retrospective audit of patients >18 yrs Time period ~ January 2008 ~ August 2008 Neutropenic fever secondary to chemotherapy (neutrophils <1.0 x 10⁹/l) The study group included patients with solid tumours only Relevant data collection tool devised Data extracted from health records Data analysed using Microsoft Access Total sample size N21 St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09
Results 58% of patients classified as high risk 42% of patients low risk The majority of patients - lung (38%) and breast (42%) primary Carbo/gem (23%), taxotere (14%), AC (23%) Length of stay ↑ high risk (6days compared to 4days) 76% a/b’s given within 4hr target Length of antibiotics – equal for high and low risk Less IV days for low risk St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09
Conclusions St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09 Pathway still not perfect but has improved the care for patients It encourages better communication and awareness of A&E staff
Recommendations:The Future St Helens & Knowsley Teaching Hospital NHS Trust ~ CGARRD 2008-09 • Re-audit in 1 year • Reduce length of stay for low risk patients by facilitating early oncology referral / safe early discharge • Thorough education to ensure safety • Use of tools • Responsibility • Link nurse with A&E • Chemo alert