Download
1 / 37
380 likes | 658 Views
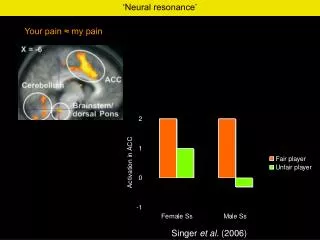
PAIN. “Its All in Your Head” Michael Raucci D.C., D.I.B.C.N. Board Certified Chiropractic Neurologist International Academy of Chiropractic Neurologists. Pain. The unpleasant awareness of a noxious stimulus or bodily harm. Pain. Where is the Pain? In the Hand?. The Mystery of Pain.

E N D
PAIN “Its All in Your Head” Michael RaucciD.C., D.I.B.C.N. Board Certified Chiropractic Neurologist International Academy of Chiropractic Neurologists
Pain • The unpleasant awareness of a noxious stimulus or bodily harm
Pain • Where is the Pain? • In the Hand?
The Mystery of Pain • Where is the pain now? • In the hand? • Nociception • Pain Perception
The Phantoms Within Us Phantom Limbs
Not Everything Works the Way you Would Expect • Body maps • Distortion • Implications in Athletics • Digit synesthesia
Fibromyalgia • Pain in the muscles • Severe Fatigue • Depression/Anxiety • Deconditioning Brain Disorder of Pain Perception
Anorexia Nervosa and Bulemia • Body Image • Neuronal Connections Brain Disorder of Body Map/Image Perception
“Neurons that Fire Together, Wire Together” • Neurons that fire apart, wire apart • Associative connectionism
Media Violence • The core network • The ethics network
For the most part, similar regions of the brain are activated, corresponding to the visual and auditory areas of the brain. But when we look at the difference between violent and non-violent scans, those areas are mostly cancelled out, and we are left with images showing the differences between viewing violent and non-violent videos. • The next set of images shows only the difference between the violent and non-violent videos, which was the focus of this study. • The differences in the paralymbic area (marked Par) in the right hemisphere indicate that the violent videos used significantly more emotional processing. The posterior cingulate nucleus (PCg) was also activated, indicating emotional memory retrieval. The hippocampus (Hipp) activation indicates episodic memory storage, suggesting violent videos are more likely to be remembered. Finally, the right amygdala (Amg), the center of the fear reflex, was also activated. • Murray et al. argue that the activation of primitive regions of the brain such as the amygdala suggest that though children may be aware that violent media present no real danger, their brain's response is identical to situations when a real threat is present. The amygdala is also active in impulsive aggressive individuals, suggesting that children may have little control over their response to violent media. Since long-term memory regions are also affected by violent videos, it's possible that the effects of the videos extend beyond the viewing period.
The Rich Environment Not Rich Rich
The Safe Environment • The role of the unconscious • The Role of the Amygdala • Flashing pics • Fear pathways “I Love Puppies”
Mirror Neurons LEFT – PERFORMING AN ACTIVITY RIGHT – THINKING ABOUT THE SAME ACTIVITY Imitation is a strong form of learning
Mirror Neurons • Swinging baseball bat • Watching someone swing a baseball bat • Imagining swinging a baseball bat • Reading about how to swing a baseball bat • Imparting skills
#1 Symptom • Pain is overwhelmingly the reason people seek medical care • Training and the understanding of pain is grossly unsatisfactory at healthcare training institutions • Pain is a subjective complaint without an objective test • Pain thresholds and tolerances vary greatly from person to person, and culture to culture
Types of Pain (Quality) • Sharp • Dull • Throbbing • Tearing • Squeezing • Cramping • Burning • Nauseating • Shooting • Heavy • “worst headache of my life”
Types of Pain (Locality) • Neuropathic • Nociceptive • Central • Sensitization • Psychogenic • Superficial • Somatic • Deep Somatic • Visceral
Referred and Radicular Pain • Referred pain is pain that is present in a site other than where the injury is because of shared or adjacent neurologic structures in the afferent pain pathway (This often is the result of spillover in the dorsal horn of the spinal cord or adjacent structures in the brain) • Radicular Pain is perceived as distal to a nerve irritation in the served neurotome or dermatome.
Gate Theory • Melczak and Wall • “The perception of pain is not a direct result of activation nocicpetors, but instead is modulated by interaction between neurons, both pain-transmitting and non-pain-transmitting.” • The signal passes through gates which have the capacity to inhibit/dampen the signal
Small nerve fibers (pain receptors) and large nerve fibers ("normal" receptors) synapse on projection cells (P), which go up the spinothalamic tract to the brain, and inhibitory interneurons (I) within the dorsal horn. • The interplay among these connections determines when painful stimuli go to the brain: • When no input comes in, the inhibitory neuron prevents the projection neuron from sending signals to the brain (gate is closed). • Normal somatosensory input happens when there is more large-fiber stimulation (or only large-fiber stimulation). Both the inhibitory neuron and the projection neuron are stimulated, but the inhibitory neuron prevents the projection neuron from sending signals to the brain (gate is closed). • Nociception (pain reception) happens when there is more small-fiber stimulation or only small-fiber stimulation. This inactivates the inhibitory neuron, and the projection neuron sends signals to the brain informing it of pain (gate is open). Descending pathways from the brain close the gate by inhibiting the projector neurons and diminishing pain perception. • This theory doesn't tell us everything about pain perception, but it does explain some things. If you rub or shake your hand after you bang your finger, you stimulate normal somatosensory input to the projector neurons. This opens the gate and reduces the perception of pain.
Why do we have Pain • Pain is an evolutionarily important phenomena because it encourages an organism to disengage from a noxious or self-damaging stimulus, direct attention to an injured area, and promote healing.
Acute, Subacute, Chronic Acute – day 1-3 - frank inflammation, sharp pain Subacute – day 3-30 Chronic - 3+months
Chronic Pain • Is more than a symptom. It is an illness in itself. Pains effect on attention
Ice or Heat • Rule #1 – You’re never wrong if you use ice • Rule #2 – Ice a new or inflamed injury • Rule #3 – Heat a muscle spasm when there has been no injury
Mobilize or Immobilize • When appropriate mobilize ASAP • Healing along lines of stress • Immobilize when there exists instability
(P)RICE • Protect • Rest • Ice • Compression • Elevation