Download
1 / 40
470 likes | 995 Views
CNS Physiology. Review. Electrophysiology. Length constant - distance along membrane at which voltage signal is reduced to 37% of its original amplitude Time constant - amount of time it takes to reach 63% of membrane steady-state voltage. Electrophysiology.

E N D
CNSPhysiology Review
Electrophysiology • Length constant - distance along membrane at which voltage signal is reduced to 37% of its original amplitude • Time constant - amount of time it takes to reach 63% of membrane steady-state voltage
Electrophysiology • Temporal Summation - determined by time constant - larger the time constant of postsynaptic cell, the longer it lasts and the greater the extent of temporal summation • Spatial Summation - determined by length constant - larger the length constant, the more “potent” the potential when it reaches axon hilloc (more efficient electronic conduction)
Metabolic & Circulatory Features • Gases, water, small MW compounds & lipid-soluble molecules can diffuse across BBB • High MW compounds and polar molecules can NOT diffuse across BBB • Glucose, amino acids, pyruvate, ketones, etc. cross via active transport
Metabolic & Circulatory Features • Capillary endothelium = BBB (glia surround endothelium) • BBB can be breached by using a hyperosmotic sucrose solution to shrink endothelial cells and loosen the tight junctions • Smoking is also an effective method of breaching BBB (~20% blood in lungs goes straight to brain)
Metabolic & Circulatory Features • Monro-Kellie Doctrine - an increase in any component in calvarium (tumor, edema, CSF blockage) must be accompanied by a decrease in another component • Cytotoxic edema - intracellular edema caused by ischemia - ion pumps shut off and cells swell - BBB intact • Vasogenic edema - extracellular edema caused by hemorrhage - BBB permeability increased • Both types of edema lead to cell death
Metabolic & Circulatory Features • Mean cerebral blood flow doesn’t vary with BP under normal circumstances • When blood flow does change, it changes in relation to metabolism (lots of active pumps - lots of energy needed) • Exception - Hypercapnia!!! - when pCO2 increases, BP increase
Metabolic & Circulatory Features • Deoxyglucose - passes through glucose pumps but isn’t metabolized • PET scan - uses flourodeoxyglucose (F18) probe - high energy radioactive material with short T1/2 - more metabolically active cells take up more F18 - images energy utilization • SPECT scan - uses lipid soluble probe (HMPAO) w/ longer T1/2 than F18 - diffuses across cell then is demethylated (trapped) - measures blood flow • fMRI - uses blood oxygen dependent level (BOLD) contrast - detects oxygenated vs. deoxygenated Hb - activity measured by deoxyHb replacing oxyHb
GLU and GABA Synthesis • Glu GABA utilizes cofactor PLP • Deficiencies in B6 lead to inhibited GABA synthesis causing convulsions (decreased inhibition) • Thiazide diuretics can be a cause of B6 deficiency PLP
Acetylcholine Synthesis • ACh synthesis is substrate limited (ie dependent on the [choline]) • Uptake of choline is regulated making it hard to increase Ach (instead drugs are used to inhibit the breakdown of Ach) +
Catecholamine Synthesis • Limited by [tyrosine] • Regulated by end product inhibition of tyrosine hydroxylase • Tyrosine hydroxylase is also dependent upon tetrahydrobiopterin (THB) - when TH is phosphorylated, its affinity for THB increases • Epi synthesis utilizes SAM to get methyl group (corticosteroids upregulate this) TH
More NT Synthesis • Serotonin Synthesis • Limited by [tryptophan] • Insulin increases the transcription of transporters that selectively uptake Phe and Tyr as oppose to Trp such that Trp is more available in the blood • Melatonin Synthesis • Breakdown product of serotonin • Activated by darkness • Neuropeptides • Regulated by gene transcription
NT Release • Electrical Aspects • Ca+2 dependent - amount of Ca+2 released proportional to NT release • Tetrotoxin - blocks Na+ channels - blocks presynaptic activity - no Ca+2 released - no vesicles released • K+ channels are poisoned - sustained release b/c can’t restore RMP • Molecular Aspects • Synapsin brings vesciles to the membrane • Ca+2 phosphorylates synapsin releasing the vesicle • SNAREs & SNAPs aid in vesicle fusion
NT Receptors • Ach • Nicotinic • Cation Channel (Ca++ in CNS) • Spinal Cord, Sup. Colliculus • Muscarinic • G-protein-coupled, Gi inactivates Adenylate Cyclase, Gq activates PLC- Ca++ influx • M1- striatum, hippocampus, cerebrum • M2- cerebellum
NT Receptors • GABA • GABAA • Postsynaptic Cl- channel - reinforces the RMP • Agonists- inhibition. Prevents NT release Muscimol, Barbs, (Benzos) • GABAB • G-protein-coupled, activates Adenylate Cyclase • Axoaxonal GABAB - PRE POST GABAA -
Somatosensory • Mechanoreceptors (Ab afferents) • MOA: pressure stretches membrane and opens Na+ channels causing Na+ to flow into cell • Stimulus intensity is proportional to receptor potential • Coded by frequency of firing • Slow Adapting - Touch and Pressure - prolonged stim • Merkel’s Disk - detect location of stimulus • Ruffini Corpuscles • Fast Adapting - Touch - onset/offset stim • Meissner’s - detect low-freq. vibrations or flutter • Pacinian Corp. - detect high frequency - • Hair follicle - velocity detector • Proprioception • Muscle spindles - detect ∆ length • Joint receptors - detect position, direction & velocity of movement
Somatosensory • Afferent Fiber Types • Ia > Ib > II = A > A > C • All proportional to fiber diameter • In general, deeper the receptor in the skin the larger the receptor field • DCML • 1 - skin to dorsal horn up gracile or cuneate fascile to medulla • 2 - up ML to thalamus to synapse VPL or VPM • 3 - up post. IC to synapse in somatosensory cortex (312)
Somatosensory • Pain • Detected by nociceptors (free nerve endings) • Prolonged or repetitive activation of pain receptors makes them more sensitive • Pain response • Sensory - detected by nociceptors • Behavioral - active, passive or nonavoidance • Autonomic - severe pain (SNS response) vs. visceral pain (PSNS response) • Motor - w/drawl or guarding (visceral)
Pain - Receptor Specificity • Nociceptors - detect mechanical, heat or chemical stimulation • Fast (1st) pain - A fiber - smallest mylenated fiber that senses localized pain or heat > 45C • Slow (2nd) pain - C fiber - unmylenated that senses poorly localized pain • More C fibers than A fibers • C fiber response outlasts stimulus • Thermoreceptors - detect temp < 45C • Cold (A & C) • Warm (C) • Itch Receptors (C) • Activated by histamine
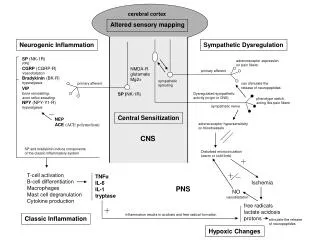
Physiology of Pain • Damage to cell releases K+ which depolarizes cell and activates nociceptor leading to release of substance P and CGRP (calcitonin gene related peptide). • Substance P acts on mast cells to evoke degranulation causing release of histamine potentiating the nociceptor. • CGRP dilates blood vessels causing edema and release of bradykinin further potentiating nociceptor
Somatosensory • Spinothalamic System (ALS) - fast pain - 1 A fibers synapse on lamina V dentrites in lamina IV and are inhibitory (massage inhibition) • Spinoreticular System - slow pain • Spinomesencephalic - emotional & autonomic affects of pain
Axon Reflex • Mediated by C fibers • W/in 30 sec, C fibers transmit signal back out to periphery causing release of substance P which dilates blood vessels leading to red flare Triple response: Red rxn - from direct stim - from bleeding/dilation Wheal - from increased histamine & capillary permeability - edema Red flare - axon reflex (subP) p p p Type C
Somatosensory • Nociceptive Fibers (Ad or C)synapse on SC neurons in the anterior horn (A). • Descending 5-HT or NE neurons can modulate these synapses to prevent pain transmission. • Lesions in any part of the descending pathway will cause temporary hyperalgesia
Auditory Physiology • Sensory Transduction • Movement of basilar membrane causes deflection of stereocilia against tectorial membrane • Deflection toward tallest stereocilia causes K+ channels to open (depol) • Endolymph - high in K+ • Depolarization opens Ca+2 channels releasing NTs and opening Ca+2-dependent K+ channels causing K+ to flow back out and repolarize the hair cell • Perilymph - low in K+ • Pitch Perception • Location of highest amplitude deflection on basilar membrane is factor for coding pitch • Each hair cell is tuned to a resonance frequency • Electrical tuning - placement along basilar membrane • Mechanical tuning - stiffness/flacidness of hair cell - (stiffer near base)
Auditory Physiology • Hair Cells • Inner Hair Cells • short, stiff stereocilia • Receive more afferents - predominant role in transfer of auditory info to CNS • Outer Hair Cells • Receive input from CNS that can change membrane potential (change amplitude) • Efferents to OHCs release ACh onto OHCs hyperpolarizing them and decreasing their motor output causing suppression of sensory response and elevating auditory threshold
Neural Coding of Pitch • Phase locking - @ lower frequencies (<500Hz) firing in individual auditory fibers can phase lock to frequency of stimulus - direct coding • Volley Principle - codes higher frequencies that are too fast for phase locking - summation • Place Principle - also codes high frequencies - utilizes tonotopic mapping of basilar membrane
A lesion above what level of the auditory pathway will result in problems localizing sound?
Answer: Superior Olivary Nucleus • 1- spiral ganglion to cochlear nucleus • 2- info to both superior olivary nuclei • 1st binaural input • 3- inferior colliculus • 4- medial geniculate nucleus (thalamic relay) • 5- primary auditory cortex on superior temporal gyrus (41 & 42)
Auditory Physiology • Perception of Loudness • Depends both on amplitude and frequency b/c minimum sound intensity varies with frequency of sound (Equal Loudness Contours) • Sound Localization • Loudness difference between the two ears is detected by the LSO (high freq) • Phase difference between the two ears is detected by the MSO (low freq)
Vestibular System • Hair cells - similar to those in cochlea w/ addition of kinocilium • Basal firing of vestibular nerve occurs in absence of any stimulus allowing bidirectional regulation • Semicircular Canals • Measures angular acceleration through pressure change exerted on cupula by endolymph in canal • Endolymph lags behind initial movement and thus exerts a force in opposite direction of head rotation • Vestibulo-ocular reflex - head moves to one side and eyes move to other • Utricle & Saccule • Monitor static head position and linear acceleration • Utricle - horizontal - fire when supine • Saccule - vertical - fire when upright
Vestibular System • Vestibulospinal - balance & posture • Pathology - ataxia • Vestibulocerebellar - reflexes & balance • Vestibulo-ocular - eye movements • Pathology - abnormal nystagmus • Vestibulo-cortical - conscious awareness of position • Pathology - dizziness/vertigo • Vestibulo-autonomic - correlating visual and vestibular information • Pathology - motion sickness
Spinal Reflexes • Stretch Reflex • Sensor = muscle spindle • Stretch activates Ia fibers • Ratio of intrafusal to extrafusal fiber determines how fine movement can be (lower ratio - finer movement) • Golgi Tendon Organ • Senses tension • Ib fibers synapse on inhibitory internerurons • Synaptic delay depends on # synapse in reflex arch • Muscle Spindle • Ia - annulo-spiral endings - respond to rapid ∆ • II - flower spray endings - most active when stretched to limit - proprioceptive info • - efferent mn innervating intrafusal mn in spindle • Reciprocal Inhibition • Ia afferents innervate both synergistic and antagonistic muscle • GTO excites inhibitory interneuron which relaxes antagonist muscle • Renshaw cell - gives feedback inhibition on agonist and activation of antagonist when mn is overactive
Basal Ganglia Disturbances • Parkinsonism • Degradation of dopaminergic neurons in substantia nigra • Resting tremor, akinesia, bradykinesia, cogwheel rigidity • Huntington’s Chorea • Loss of GABA due to med. Spiny neurons (caudate atrophy) • Inhibition of indirect loop • Chorea, dementia, deceased tone • Ballism • Damage to subthalamic nucleus - inhibition of indirect loop • Flailing movements • Athetosis • Damage to GP and Putamen • Wormlike, writhing movements, dystonia (posture issues) • Doesn’t go away with sleep • Tardive Dyskinesia • Iatrogenic side effect of antipsychotic drugs (thorazine) • Involuntary mouth movements due to supersensitivity of DA receptors (buccolingual dyskinesia)
Cerebellum • Neurons - all inhibitory (GABA) except Granule Cells (glutamate) in parallel fibers that synapse of purkinje cells • 3 regions of cerebellum • Cerebrocerebellum • dentate nucleus • Planning & initiation • Spinocerebellum (vermis & intermediate region) • Vermis - fastigial nuclei - medial muscle control • Intermediate - interposed nuclei - lateral muscle control • Vestibulocerebellum (flocculonodular lobe) • Vestibular nuclei • Vestibulospinal - posture • Occulomotor - head and eye movements
Cerebellar Lesions • Lesions - damage is always same side! • Cerebellar Damage • Intention Tremor • Ataxia • Delayed Initiation • Dysmetria (inaccuracy in range & direction)
Decoricate vs. Decerebrate Rigidity • Decorticate: CNS Damage above level of Red Nucleus • Rubrospinal Tract active- activates arm flexors with response to pain or head turn in contralateral direction • Decerebrate: CNS Damage at or below level of Red Nucleus • Everything extended except fingers.
Reticular Formation • Serotonin • Raphe Nuclei - descending pain & sleep/wake • Dopamine • SN - nigrostriatal path (direct loop) • VTA - reward pathway • Norepi • Locus Coeruleus - arousal & selective attention • Silent during REM • ACh • Pedunclelopontine & LDT - sleep/wake • Active during REM • Basal Forebrain - memory • Degenerates in Alzheimers
Sleep-Wake Cycle • REM • Sawtooth waves, mixed frequency EEG • Dreaming, Paralysis • NREM • Stage 1 – Low voltage, mixed freq • Stage 2 – Sleep spindles, K complexes • Stage 3 – Delta waves • Stage 4 – More Delta waves • Reticular Nucleus - inhibitory to all thalamic nuclei • Wakefulness - reticular nucleus is inhibited by cholinergic neurons, locus coerulus & raphe • NREM - reticular formation dominant • REM - cholinergic neurons only inhibit RN
Visual System • Light changes 11-cis retinal to: • All-trans retinal • This activates: • Transducin • This activates • Phosphodiesterase • This changes: • cGMP to GMP • This causes: • Cation channels to close - hyperpolarization • Channels open to Na+ and Ca+2 • Visual sensation - cessation of NT release (photoreceptors most active in dark) • Retinal pigment epi - restores 11-cis retinal