Download
1 / 10
100 likes | 222 Views
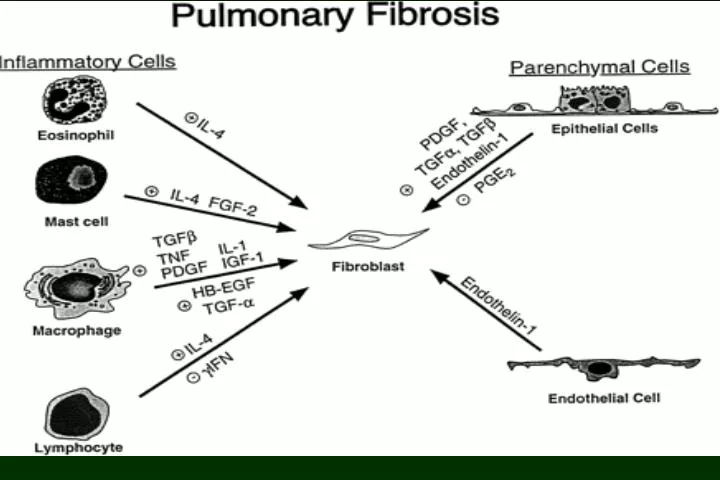
Lung Inflammation. IFN - g Receptor. TGF - b Receptor. Th1. Th2. ELR- CXC. ELR+ CXC. Cellular Phase. Fibrotic Phase. Ground Glass Consolidation Micronodule. Linear, Reticular , Reticulo-nodular Honeycombing, Cystic. DIP, NSIP. UIP. Consider steroid. Consider others.

E N D
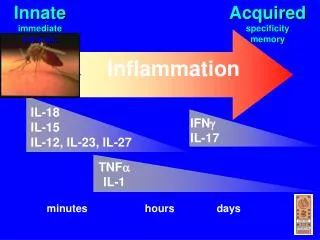
Lung Inflammation IFN - g Receptor TGF - b Receptor Th1 Th2 ELR- CXC ELR+ CXC Cellular Phase Fibrotic Phase Ground Glass Consolidation Micronodule Linear, Reticular , Reticulo-nodular Honeycombing, Cystic DIP, NSIP UIP Consider steroid Consider others
Clinical Features of ILD • Progressive dyspnea and cough, and abnormal chest radiograh, and impaired pulmonary function test • 5%-10% have normal chest film: but abnormal findings in HRCT and bronchoalveolar lavage • Normal flows , volumes , and DLCO but abnormal exercise testing
Symptoms • Dyspnea: most common • Cough • Substernal chest pain
Imaging Studies of ILD • Chest radiograph: diffuse reticular or reticulonodular markings prominent in the lower lung, Early, a hazy “ground glass”-acute alveolitis, Later curvilinear strand predominate and may coalesce into nodular infiltrates. End-stage: linear opacities are seen in all lung fields, the lung fields appear contracted, and ring-shaped opacities resulting from cystic and bronchietatic changes are obvious, creating the honey-combed appearance
Diffuse Lung Diseases • Ground Glass Lesion • Consolidation (airspace filling) • Micronodular • Linear • Reticular • Reticulo-nodular • Honeycombing or multi-cystic
Ground Glass Opacity 李昆翰 CML GVHD 2715478-5
Perilymphatic & Centrilobular Nodules: Silicosis Perilymphatic Centrilobular Webb: 104
DLD with Linear & Reticular Patterns Webb: 72