Download
1 / 42
430 likes | 515 Views
Explore the definitions, pathogenesis, and reactions of inflammation in the lower respiratory tract, focusing on acute and chronic inflammation processes. Learn about related infections, routes of infection, predisposing factors, and the microorganisms involved.

E N D
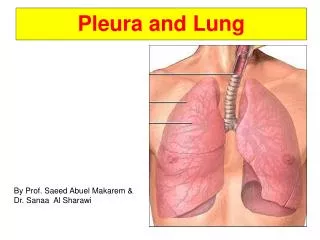
InflammationLung parenchyma & pleura Soheir Mahfouz
Definition of Inflammation It is a vascular & cellularreaction of the living tissuetoinjury. In an attempt to localize, destroy & remove the injurious agent to make way for repair
PATHOGENESIS LOCAL REACTION • Regional lymphangitis & lymphadenitis • necrosis & degeneration + inflammation SYSTEMIC • Fever • Malaise • Bood changes: -Leukocytosis -Immune reaction -Bacteria in culture
MICROSCOPIC Celluar exudate: PNLs & macrophages Fluid exudate : Edema & fibrin Vascular Dilated congested BV GROSS Swelling Increased size & weight Redness BASIC REACTION ACUTE INFLAMMATION
A) SUPPURATIVE Localized: Abscess Diffuse: septic Bronchopneumonia confluent pneumonia B) NON SUPPURATIVE Catarrhal. Pseudomembranous Mucosal Tracheobronch Fibrinous/serofib/serous mesothelial cavities: pleura Necrotizing Hemorrhagic Allergic Lung & bronchial tree ACUTE INFLAMMATION
CHRONIC INFLAMMATION DEFINITION: Reaction of living tissues to injury, which has a gradual onset & prolonged duration. The cell injury goes hand in hand with the repairprocess.
A) SPECIFIC Localized: Granuloma B) NON SPECIFIC Localized----abscess Diffuse:Occurs following acute inflammation CHRONIC INFLAMMATION
MICROSCOPIC Celluar exudate: lymphocytes, plasma cells & macrophages Fibrosis Endarteritis obliterans BV GROSS Shrinkage Whitish tough tissue with smooth surface Palour BASIC REACTION CHRONIC INFLAMMATION
Important terms in inflammation • Acute inflammation is a stereotyped response to recent or ongoing injury. Although the process is complex, the principal features are dilatation and leaking of vessels, and involvement of circulating neutrophils. • You can recognize neutrophils in tissue sections by their segmented nuclei. Pus is neutrophils plus liquefaction necrosis. Usually, the neutrophils themselves caused most of the necrosis.
Important terms in inflammation • Chronic inflammation ("late-phase inflammation") is a response to prolonged problems, orchestrated by T-helper lymphocytes. It may feature recruitment and activation of T- and B-lymphocytes, macrophages, eosinophils, and/or fibroblasts. Again, the process is complex. You will recognize lymphocytes in tissue section by their small, "blue button" nuclei. • Granulomas are seen in certain chronic inflammation situations. They are clusters of macrophages which have stuck tightly together, typically to wall something off. Such macrophages are called epithelioid cells. You will recognize granulomas in tissue sections by their characteristic appearance, or the presence of giant cells.
Important terms in inflammation • Fibrin is fibrinogen released from damaged vessels, and activated by the clotting cascades when blood meets tissue juices. Fibrin forms the meshwork which controls bleeding, and then becomes the framework for fibroblasts and angioblasts which will form the scar. Until the new scar is complete, the whole meshwork of immature scar is called granulation tissue. When the scar has matured, it contracts.
INFECTION Are inflammations caused by microrganisms
INFECTIONS OF LUNG • In lower respiratory tract - Bacterial infections cause pneumonia (lobar or bronchopneumonia) or abscesses & empyema. - Viruses cause interstitial inflammation (pneumonia) - Fungal & mycobacterial infections are mostly granulomatous NB: Atypical pneumonia is a clinical term applied to pts with an acute febrile presentation & patchy interstitial infiltrates without alveolar exudates
ROUTE OF INFECTION • Inhalation-Aspiration • Hematogenous dissemination from distant sites of infection • Direct extension from proximal sites
In immunocompetent hosts 1- Following upper respiratory tract infection 2- Smoking or inhalation of toxic fumes 3- Alcohol & sedatives diminish reflexes 4- Cold dry air & medications cause viscous mucous 5- industrial fumes & chronic Bronchitis increase goblet cells & alter ciliary function 6- Obstruction of airways prevent clearance with stagnation In immunocompromised hosts 1-Primary immunodeficiency 2-Secondary : acquired immunodeficiency - T/ B cell defects - Monocyte or granulocyte dysfunction or a combination - Iatrogenic PREDISPOSING FACTORS
POPULATIONS AT RISK • Infants & children • Elderly • Postoperative • Unconscious patients • Immunodeficiency • Pulmonary edema • Smokers • Children with genetic disorders
MICROGANISMS • Bacteria • Fungi • Viruses • Mycoplasma • Protozoa
MICRORGANISMS & other causes The frequency of infection with a certain organism relates to the site of acquisition, virulence, dose & immune status • Community acquired: Viral –Influenza, Respiratory scyncetial v. Bacterial- Pneumoniae, H.influenza etc… Non infectious: Aspiration p.-Lipid p.-BOOP-Eosinophylic pneumonia pneumonia- UIP • Hospital acquired (Nosocomial): Resistant bacteria-Staph, Klebsiella, pseudomonas Fungal-Candida, Mucor Viral-Cytomegalovirus & varicella Parasitic- Pneumocystis carinii • Others: SARS- Pneumocystis carinii- UIP- Chronic pneumonia (granulomatous)- pneumonia in immunocompromised host.
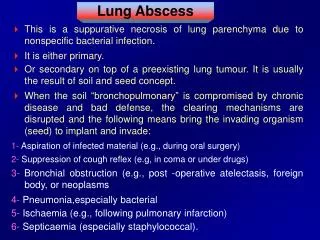
PARENCHYMAL INFLAMMATIONS • Pneumonia and ILD • Lung abscess • Granuloma
PNEUMONIA DEFINITION: Patchy or diffuse , inflammation/infection of the lung parenchyma TYPES ACCORDING TO DISTRIBUTION • Lobar : Bacterial, whole lobe affection • Bronchopneumonia: Bacterial, patchy distribution • Interstitial: Viral, little or no alveolar space exudation • Segmental: like lobar p. but involves part of a lobe • Granulomatous pneumonia: mycobacterial & fungal
CAUSATIVE AGENT Bacterial Mycoplasma Legionella Chlamydia Viral Fungal Protozoal MODE OF EXPOSURE Postoperative Postinflammatory / embolic Postobstructive Postinfluenzal (s. aur) Aspiration Ventilator associated Immune mediated PNEUMONIATypes according to
MISCELLANEOUS pneumonia • Acute febrile pneumonia of infancy • Neonatal pneumonia • Community acquired pneumonia CAP* • Eosinophilic pneumonia • Cryptogenic pneumonia • Non resolving pneumonia • Recurrent pneumonia • Atypical pneumonia (pneumonitis) • Walking pneumonia • Extrinsic alveolitis
LOBAR PNEUMONIA DEFINITION: Acute diffuse fibrinous inflammation of the alveoli, uniformly occurring in one or more lobes of the lung in Community aquired pneumonia (CAP) caused by Strept. Pneumoniae (pneumococci) Klebsiella in alcoholics Legionella.
LOBAR PNEUMONIA ETIOLOGY & PATHOGENESIS • Organism: Strept pneumonia (pneumococci)- Klebsiella -Legionella • Route: Air born by droplet infection Occurs in previously healthy young individuals & middle aged people (Organism is highly virulent, spreading rapidly through pores of Kohn) producing CROSS COUNTRY filling
Lobar pneumonia – Stage of congestion 12-24 hrs • Congested edematous alveolar walls • Alveolar space containing RBC’s – organism & edema fluid
Lobar pneumonia – Stage of resolution 2-5 days • Macrophages clear area with restitution of normal pulmonary architecture • NB with the advent of antibiotics, there is alteration of the inflammatory repair mechanisms resulting in organization & fibrosis instead of resolution
Lobar pneumonia – Complications • Most cases heal by resolution • Healing by fibrosis or carnification • Postpneumonic abscess • 20-30% get bacteremia & die despite antibiotics
ACUTE LUNG ABSCESS postpneumonic
Lobar pneumonia – CP • Fever chills & productive cough • Sputum watery to rusty in advanced cases • Dyspnea & cyanosis • Pain & friction rub
Lobar pneumonia - Diagnosis • Clinical evaluation: CP in 80% of pts • Laboratory: Sputum >25 PNLs & few / no epith cells- culture +ve(Gm +ve diplococci) Blood: Leukocytosis(15-30,000)+ shift to left* • Radiographic : chest X ray • Microbiologic : blood , sputum & trans bronchial culture & sensitivity