Download
1 / 31
320 likes | 334 Views
Explore the intricate anatomy and physiology of the urinary system, focusing on the kidneys and nephrons' role in urine formation and filtration. Learn about the structures like ureters, urethra, and renal capsules, and the process of blood supply, tubular reabsorption, and glomerular filtration.

E N D
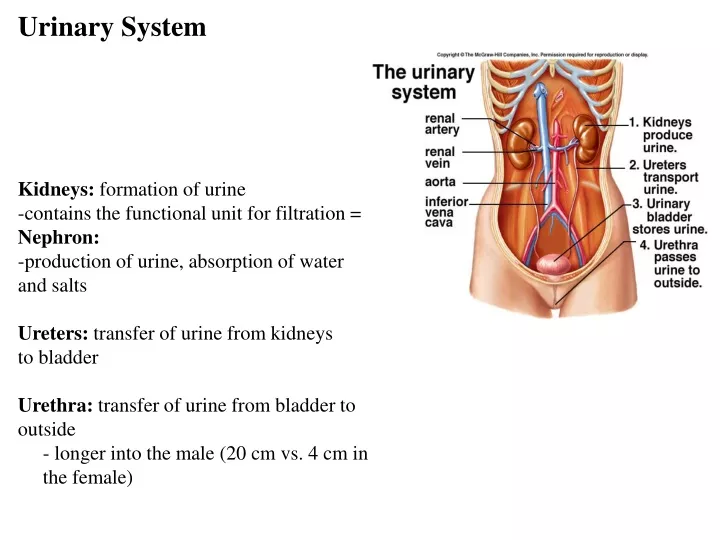
Urinary System Kidneys: formation of urine -contains the functional unit for filtration = Nephron: -production of urine, absorption of water and salts Ureters: transfer of urine from kidneys to bladder Urethra: transfer of urine from bladder to outside - longer into the male (20 cm vs. 4 cm in the female)
Kidneys • 10-12 cm • retroperitoneal – behind the peritoneum • not part of peritoneal cavity • surrounded by three layers of tissue • 1. deepest layer = renal capsule – transparent sheet of dense irregular connective tissue • 2. middle layer = adipose capsule • 3. outer layer = renal fascia
Kidneys • divided internally into an outer cortex and an inner medulla • medulla consists of 8 to 18 cone-shaped regions called renal pyramids • the wider base faces towards the cortex, the narrow region (renal papilla) projects down • renal cortex is divided into an outer cortical zoneand a deeper juxtamedullary zone • the cortex also extends down in between the pyramids to form the renal columns
Kidneys Minor calyx • The renal papilla projects down into a cup-like structure called a minor calyx • Minor calyces unite to form a major calyx • All major calyces unite to form the renal pelvis Renal pelvis Major calyx Renal papilla of pyramid
Renal Papilla Renal Pyramid Minor Calyx Major Calyx Renal Cortex kidney Renal Pelvis Renal Medulla URETER URETER URETER BLADDER
The Nephron -about one million nephrons between the two kidneys -kidneys filter 180 L fluid per day!!!! -each nephron is a renal corpuscle + renal tubules -renal corpuscle: the filtering unit consisting of a tangled cluster of capillaries known as the glomerulus + the glomerular capsule -tubules: for reabsorption of water and ions leading to final urine volume and composition • Glomerular capsule (Bowman’s capsule) • Proximal convoluted tubule • Loop of Henle • Distal convoluted tubule • Collecting duct
The Nephron Path of filtrate: - Proximal convoluted tubule -> Loop of Henle -> Distal convoluted tubule -> Collecting duct -> calyces renal pelvis ureter • PCT and DCT are “covered” by a peritubular network of capillaries for reabsorption back into the blood • Loop of Henle is covered with the vasa recta capillary network Interlobular artery Interlobular vein
Blood supply • supplied by a renal artery and drained by a renal vein(s) • kidney receives 20-25% of the resting cardiac output through the renal arteries (1200mL per minute) • renal artery divides into segmental arteries– supply segments of the kidney • the segmental arteries give off branches that pass through the renal columns – interlobar arteries • at the base on the renal pyramids – between the medulla and cortex – they are called arcuate arteries • divisions from the arcuate are called the interlobular arteries
Blood supply • The interlobular arteries give rise to the afferent arterioles • afferent arteriole supplies one nephron and forms the glomerulus (capillary network) • Filtered blood flows out of the glomerulus via the efferent arteriole • efferent arteriole forms the peritubular capillary networkwhich surround the upper portions of the nephron • an extension of this network covers the lower portion of the nephron – vasa recta • the peritubular capillaries form the interlobular veins arcuate veins interlobar veins segmental veins renal vein
Cortical Nephron • 80-85% of nephrons are cortical nephrons • Renal corpuscles are in outer cortex and short loops of Henle lie mainly in cortex • Extensive capillary networks
Juxtamedullary Nephron • 15-20% of nephrons are juxtamedullary nephrons • Renal corpuscles close to medulla and long loops of Henle extend into deepest medulla enabling excretion of dilute or concentrated urine • Minimal capillaries covering nephron
Cortical Nephron Juxtamedullary Nephron
renal lobe = renal pyramid + the overlying renal cortex + ½ the adjacent renal column
Renal Physiology • 1. Glomerular filtration • water and most solutes in the blood plasma move across the glomerular capillaries into the Bowman’s capsule and then into the renal tubules • 2. Tubular reabsorption • cells lining the renal tubules reabsorb about 99% of the filtered water and many of the solutes • materials return to the blood through reabsorption into the peritubular capillary network & vasa recta • 3. Tubular secretion • tubular cells also secrete other materials – wastes, drugs, excess ions into the urine • this also removes these materials from the blood • reabsorption = return to the blood • absorption = entrance of new materials into the blood (e.g. digestive absorption)
Glomerulus • capillary tangle derived from afferent arterioles (into) and lead into efferent arterioles (out) • surrounded by a glomerular capsule (Bowman’s capsule) • glomerular capsule: site of plasma filtration and is the first step in the formation of urine • consists of visceral and parietal layers • visceral layer consists of modified epithelial cells that cover the capillaries = podocytes Visceral Bowman’s Capsule
Glomerulus • glomerular capsule: • the endothelial cells of the capillaries have spaces between them • the spaces between the endothelial cells + spaces between the podocytes forms a filtration membrane • space between the visceral and parietal layers = glomerular capsule
PCT • PCT is the site of water reabsorption (PASSIVE) - associated with the ACTIVE reabsorption of sodium ions • active transport of Na+ into the blood is by sodium pumps in the cells of the PCT • sodium pumped from inside the cells of the PCT toward the blood • chloride, bicarbonate and phosphate ions follow Na+ transport along with other cations (calcium, magnesium) = salt reabsorption • the active transport of ions into the blood plasma increases osmotic pressure within the blood • therefore water moves out of the PCT into the capillaries PASSIVELY! • PCT reabsorbs about 70% of filtered Na+, ions and water • the apical surface of the PCT epithelium forms microvilli which increases the surface area of this region
PCT • 1. active pumping of Na+ ions from inside the PCT cell into the blood (exchanged for K+) • 2. Na+ ions diffuse from urine filtrate into the PCT cell and carry glucose, chloride ions and vitamins with it • these materials the diffuse out of the cell and into the bloodstream • 3. Water passively flows after the Na+ ions 2. 2. 3. 3.
Loop of Henle • active transport of Na+ continues through the loop of Henle • descending loop of Henle is quite permeable to water but impermeable to solute movement • salt reabsorption in the ascending limb determines how much water is reabsorbed from the descending limb • ascending loop is the opposite – permeable to salt (salt pumped out of the urine back into the blood plasma) • Na+ is pumped out of the cell into the blood • causes more Na+ to diffuse into the cell – carries with it Cl- and K+ ions
DCT and Collecting Duct • DCT and collecting duct are normally impermeable to water !!!! • the DCT and CD become permeable upon action of hormones • Antidiuretic hormone – reclaims extra water to combat dehyrdation • Aldosterone – reclaims extra sodium (i.e. salt) to increase blood pressure
Collecting Duct • two types of cells found in the collecting duct: • principal cells – contain receptors for ADH and aldosterone • these receptors are also found in the DCT • binding of ADH to the principal cell increases the synthesis of aquaporins • aquaporins form water “pores” in the principal cell – more water reabsorption H20 • Aldosterone increases the synthesis of Na/K pumps – for more salt reabsorption • Blood plasma exiting the kidneys has higher than normal Na+ concentration • Results in absorption of water from tissues • Re-establishes blood volume and blood pressure
Collecting Duct • two types of cells found in the collecting duct: • intercalated cells – play a role in the maintenance of blood pH • pump H+ ions into the urine • the H+ ions combine with ammonia to form ammonium • urine is slightly acidic and smells like ammonia • the blood stays neutral
Urinary System Function 1. Water-Salt balance of blood: - water is reabsorbed into blood from the PCT, the descending Loop of Henle & from the DCT collecting duct -salt is reabsorbed from the ascending portion of Loop of Henle -with dehydration (increased blood OP) a release of anti-diuretic hormone by posterior pituitary increases reabsorption of water by cells of DCT and collecting duct -increases their production of aquaporin water channels ADHreceptor LUMEN COLLECTINGDUCT CELL ADH cAMP Second-messengersignaling molecule Storagevesicle Exocytosis Aquaporinwater channel H2O H2O
WATER BALANCE -average intake - 2.5 L (60% from drinking water, 30% from moist foods, 10% byproduct of metabolism) -regulation of intake - thirst center within the hypothalamus - e.g. as body loses water - osmoreceptors within the thirst center detects increase in osmotic pressure within the ECF – tells us to drink to decrease OP into normal range -drinking also distends the stomach which inhibits signaling from the thirst center PLUS osmotic pressure becomes normal again -water is lost through urine, feces and sweat plus respiration and skin evaporation -2.5 L of water must be lost for water balance -60% lost in urine, 6% in feces, 6% in sweat, 28% evaporation from skin and lungs -primary means of controlling water loss is through urine production
Water Balance -extracellular fluids/ECF: blood plasma, interstitial fluids, CSF, lymph etc…. -intracellular fluid/ICF: cytosol -of the 40 liters of water in the average male - 37% is ECF and 63% is ICF -blood pressure and osmotic pressure control the movement of fluid between ECF and ICF -e.g. increased blood pressure causes the movement of fluid out of the capillaries into the interstitial spaces of the tissue (between cells) – some fluid will move into the cells and become cytosol -BUT osmotic pressure causes fluids to leave the interstitial space/tissues and enter back into the capillaries
Water Balance -dehydration: blood plasma loses water (becomes more concentrated) – increase in the osmotic pressure (OP) of the plasma -OP increase is detected by osmoreceptors in hypothalamus -hypothalamus signals to posterior pituitary -posterior pituitary gland releases anti-diuretic hormone (ADH) -ADH causes distal convoluted tubule and collecting duct to increase water reabsorption back into blood and urine volume drops -BUT OP also comes back down to normal as more water is added to blood plasma -excess water intake: plasma less concentrated - decrease in OP -osmoreceptors signal to the posterior pituitary - decreases ADH release and nephrons decrease water reabsorption -urine volume goes up -OP also increases as the water content of the plasma drops
Urinary System Function 2. Acid-Base balance of blood: -dissolution of CO2 in water of cells and blood plasma produces H+ and HCO3 ions -keeps blood at a pH of around 7.5 to 7.6 -reabsorption of bicarbonate ions from urine into the blood increases levels in blood (decreases carbonic acid levels) -removal of hydrogen ions from blood by the nephron followed by its secretion into the urine – H+ combines with ammonia to form ammonium (NH4+)
Urinary System Function 3. Excretion of Metabolic Wastes:nitrogenous wastes a. Urea: by-product of amino acid metabolism -produced when ammonia + carbon dioxide -reclaim urea from bottom section of collecting duct b. Creatinine: produced by breakdown of creatine phosphate (high energy molecule reserve of muscles) c. Uric acid: by-product of nucleotide breakdown -insoluble and ppts in the blood, concentrates in joints - gout
Urinary System Function 4. Secretion of hormones: -release of erythropoietin by kidneys - stimulates RBC production by bone marrow -activation of vitamin D produced by the skin
Urinary System Function 4. Secretion of hormones: release of renin by kidneys which leads to release of aldosterone by adrenal cortex (from the zona glomerulosa layer) – increases reabsorption of salts by kidneys -leads to an eventual increase in blood volume as increased Na+ in blood “attracts” water from body tissues