Download
1 / 48
540 likes | 1.01k Views
Visual Neuroanatomy Efferent Pathways. Vivek Patel, MD University of Ottawa Eye Institute Neuro-Ophthalmology. Visual Neuroanatomy. Afferent – eye to brain Pupillary reflex arc Efferents – eye movements. Extra-Ocular Muscles. Infranuclear pathways. CN III.

E N D
Visual NeuroanatomyEfferentPathways Vivek Patel, MD University of Ottawa Eye Institute Neuro-Ophthalmology
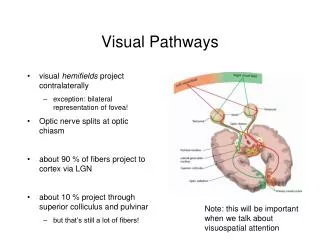
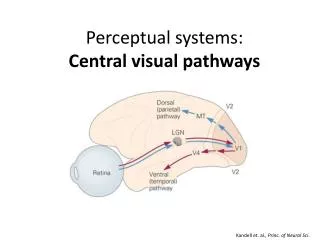
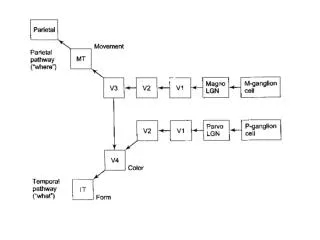
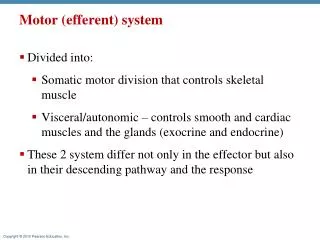
Visual Neuroanatomy • Afferent – eye to brain • Pupillary reflex arc • Efferents – eye movements
CN III • Innervates Levator, inferior oblique & all recti except lateral rectus • Projects ventrally • Enters cavernous sinus after crossing PCOM
Categorized by age Children Congenital AVM Tumor Young Adults Demyelination Vascular Tumor Older Adults Vascular Tumor CN III Injuries
CN III Subnuclei • All subnuclei are ipsilateral EXCEPT • Levator subnucleus forms a fused central nucleus • Superior rectus subnuclei decussate to innervate contralateral superior rectus muscle
IS it nuclear or peripheral ? It must be nuclear if • Bilateral CN III without ptosis • Unilateral CN III with bilateral ptosis BUT • Complete bilateral CN III • Bilateral ptosis May be either!
CN IV • Nucleus just caudal and dorsal to III • Innervates Contralateral superior oblique • Exits brainstem dorsally • Longest intracranial course
CN IV injuries • Intrinsic • Trauma • Tumor • Medulloblastoma • Ependymoma • Metastatic • Demyelination • Vascular • Congenital ( high vertical vergence amplitudes and objective excyclotorsion only) • Bilateral: V-pattern esotropia and excyclotorsion greater than 15 degrees. • Resultant compensatory head position?
CN IV injuries • Extrinsic • Tumor • Pinealoma • Metastatic • Hydrocephalus / Aqueductal stenosis
Skew Deviation? • Supranuclear cause of vertical misalignment • Does not necessarily obey the 3-step test • Ipsilateral intorsion (not extorsion as in IV palsy) • Interruption of otolith-ocular pathway at some point along it’s course
Skew deviation - OTR • Vestibulo-cerebellar: • Ipsilateral head tilt • Ipsilateral hypotropia • Excyclo of hypo eye, incyclo of hyper eye • Midbrain: • Contralateral head tilt • Ipsilateral hypertropia • Excylo of hypo eye, incyclo of hyper eye
Look for a lesion in: • cerebellum • Pons • midbrain
Normal counter-roll R IV palsy Ocular tilt rxn (skew)
CN VI • Innervates ipsilateral lateral rectus • Interneurons to contralateral medial rectus via MLF • Runs near: • CN VII • MLF and PPRF • Vestibular Nuclei • Peduncle
CN VI • Origin: ponto-medullary junction • Projects ventrally along clivus • Tethered at apex of the petrous bone by petroclinoid ligament • Enters Cavernous sinus
CN VI Injuries • Vascular • Anterior inferior cerebellar or paramedian perforators • Demyelination • Trauma • Tumor
Cavernous Sinus • Site of multiple cranial nerve palsies • Vascular • Tumor • Idiopathic • Tolosa-Hunt
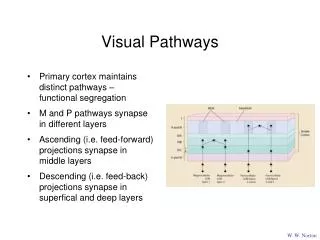
Internuclear Pathways • MLF • PPRF
Paramedian Pontine Reticular Formation • Horizontal Gaze center • Initiates horizontal eye movements • Bilateral, within Pons • Projects to ipsilateral CN VI nucleus • Lesions of the PPRF cause ipsilateral gaze palsies • PPRF lesions do not affect oculocephalic & caloric reflexes
MLF • Midbrain to cervical spine • Composed of interneurons – ipsilateral CN VI to contralateral CN III. • fascicle for horizontal gaze and vertical gaze that connects the VI and III nuclear complexes. • Trochlear nerve and otolith ocular pathways also use the MLF
Vertical Gaze • Rostral Interstitial nucleus of the MLF (riMLF) (gaze initiation) • Interstitial Nucleus of Cajal (INC) (gaze holding) INC riMLF
Upgaze • Lateral riMLF projects to contralateral inferior oblique and superior rectus sub-nuclei • Remember Superior Rectus fascicle decussates
Downgaze • Medial riMLF projects downward to ipsilateral superior oblique and inferior rectus sub nuclei • Remember the CN IV fascicle decussates • Vertical gaze is initiated by Bilateral activation of the riMLF and INC.
Alternating cover testing • Cover / uncover testing • Quantifying a deviation
Benedikt’s • Involves Red Nucleus • Ipsilateral CN III • Contralateral involuntary movements
Weber’s • Involves Cerebral peduncle • Ipsilateral CN III • Contralateral Hemiparesis
PPRF lesion • Ipsilateral gaze palsy • Provides the supranuclear input to the abducens nuclear complex. • Isolated PPRF lesion will preserve the oculocephalic and caloric reflexes.
PPRF & Nuclear sixth • Ipsilateral Gaze palsy with • Abnormal oculocephalic and caloric testing
1 and ½ syndrome • Lesion of PPRF, CN VI nucleus, MLF • Ipsilateral gaze palsy with • ipsilateral INO