Download
1 / 69
760 likes | 1.1k Views
Cardiomyopathies Andre Keren, MD. דר' ישראל גוטסמן מערך הלב, הדסה עין כרם. Cardiomyopathies. Cardiomyopathies: Heart muscle disease A myocardial disorder in which the heart muscle is structurally and functionally abnormal in the absence of:

E N D
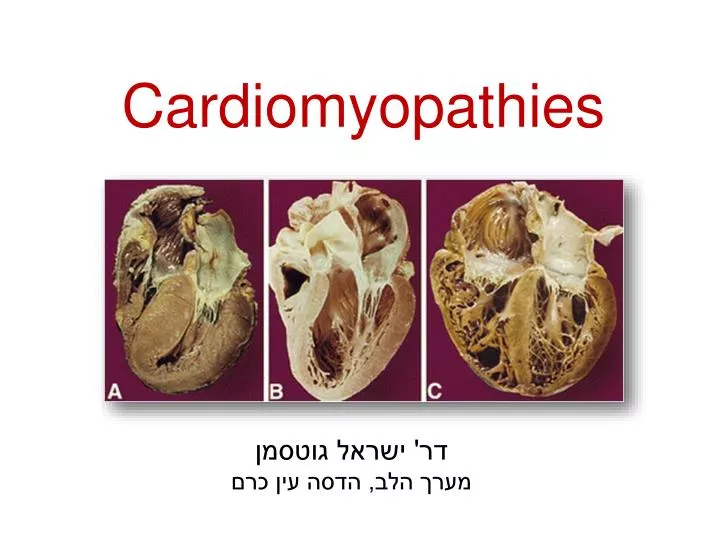
Cardiomyopathies Andre Keren, MD דר' ישראל גוטסמן מערך הלב, הדסה עין כרם
Cardiomyopathies • Cardiomyopathies: Heart muscle disease • A myocardial disorder in which the heart muscle is structurally and functionally abnormal in the absence of: coronary artery disease, hypertension, valvular disease and congenital heart disease
Cardiomyopathies • Dilated CM(DCM) • Hypertrophic CM (HCM) • Restrictive CM (RCM) • Arrhythmogenic RV dysplasia (ARVD)
Classification of Cardiomyopathies Hypertrophic Dilated Arrhythmogenic RV dysplasia Restrictive
Normal • Dilated CM • (DCM) Hypertrophic CM (HCM) • Restrictive CM • (RCM)
Genetics of CMP • Genes encoding: • Cytoskeletal proteins – DCM: • Beta/delta-sarcoglycan • Dystrophin • desmin and lamin A/C (intermediate filament) • Sarcomeric proteins – • DCM/HCM: • Actin • b-myosin heavy chain • a-tropomyosin • cardiac troponin T • HCM: • cardiac troponinI • titin • myosin light chains
Genetics of CMP HCM DCM Functional alterations caused by Z-disc mutations
Hypertrophic Cardiomyopathy (HCM) • Most common genetic cardiovascular disease • Prevalence 0.2% (1:500) • Autosomal dominant trait • Gene mutations of cardiac sarcomere proteins • 18 genes and >500 individual mutations have been identified…
Genetic Mutations in HCM Spirito P, Seidman CE, McKenna WJ, Maron BJ. NEJM 1997;336:775
Major Mutations in HCM:Risk of sudden death • Beta myosin heavy chain (35%): Typical features, both malignant and benign types • Myosin binding protein C (15%): Late appearance, usually benign • Troponin T (15%): Mild hypertrophy, malignant
Non-Sarcomeric mutations that causeStorage diseases and mimic LV Hypertophy • Anderson-Fabry disease: X-linked lysosomal storage disease (a-galactosidase A) • PRKAG2 mutation Glycogen accumulation • Danon disease: LAMP2 mutation X-linked Massive hypertrophy, preexitation, malignant prognosis
Hypertrophic Cardiomyopathy (HCM) LV Hypertrophy LVOT obstruction
LV Hypertrophy HCM AO SEPTUM LV
Natural History of LV Hypertrophy Increase in LV hypertrophy after adolescence
HCM - Histopathology Normal • Myocardial Disarray • Fibrosis Small-vessel disease: Remodeled intramural coronary arteriole with thickened media and narrowed lumen
Pathophysiology Mitral valve Abnormalities Mitral Regurgitation SAM Systolic Anterior Motion of MV ASH Asymmetric septal hypertrophy LVOT obstruction Left Ventricular Outflow Obstruction (Dynamic) Diastolic dysfunction
Clinical Presentation • Sudden death – ventricular tachyarrhythmias • Asymptomatic • Chest Pain • Limited functional capacity • Progressive heart failure • Embolic stroke
Symptoms • Exertionaldyspnea, Exercise intolerance • Fatigue • Chest pain • Syncope Pathophysiology • LV outflow obstruction - elevated LV pressures and wall stress • Diastolic dysfunction - impaired LV filling due to noncompliant and thickened wall • Myocardial ischemia from the small vessel disease
Diagnosis • Examination: Characteristic findings • ECG: LVH • Echo: Most useful diagnostic tool • ECG Holter: Arrhythmias • Stress test: Blood pressure response • Catheterization: rule out associated CAD
Physical findings in HOCM Bisferiens LVOT 4 Triple MR
Maneuvers and HOCM Murmur • Murmur increase: • Valsalva maneuver • Exercise • Standing
ECG in HCM • Abnormal in 90% of patients LVH, ST-T changes, T wave inversion
Echocardiography in HCM LVH, ASH, SAM, MR
Causes of SCD in young athletes HCM is the major cause of SCD in young & in athletes
LV Hypertrophy and SCD Significant increase in SCD risk if Max Wall thickness >30mm
Risk Stratification • Risk Factors: • Cardiac arrest/sustained VT • Multiple familial SD • Unexplained syncope • Massive LVH (>3cm) • Multiple-repetitive NSVT • Abnormal blood pressure on exercise • Malignant genotype (troponinT) • End stage disease • Extensive delayed enhancement on MRI • Marked LVOT outflow obstruction (rest) ICD 11%/yr Highest (>2) 4%/yr ? Intermediate (1) Lowest (0)
Therapy • Reduce LVOT obstruction • Alleviate elevated diastolic pressures • Reduce microvascular ischemia Beta Blockers, Verapamil, Disopyramide • Atrial Fibrillation Amiodorone, Anticoagulants • Heart Failure HF therapy
Therapy Interventions to reduce LVOT obstruction: • Pacemaker (DDD): Reduces obstruction • Alcohol septal ablation • Surgical myomectomy
Septal Myomectomy in HOCM Nishimura RA. NEJM 2004;350:1320-7
Septal Ablation in HOCM NEJM 347:1307,2002 A. Keren
Dilated Cardiomyopathy (DCM) Dilated Cardiomyopathy (DCM) Normal Heart
Dilated Cardiomyopathy (DCM) • Myocarditis: Viral/ Inflammatory • Idiopathic (50%) • Genetic
Dilated Cardiomyopathy (DCM) • Sensitivity and toxins: alcohol, catecholamines, anthracyclines, irradiation • Metabolic cardiomyopathy: endocrine abnormalities, glycogen storage disease, deficiencies (hypokalemia), and nutritional disorders • General systemic disease: connective tissue disorders and infiltrative diseases: sarcoidosis and leukemia • Muscular dystrophies: Duchenne, Becker-type, myotonic dystrophies • Neuromuscular disorders: Friedreich ataxia, Noonan syndrome, lentiginosis
Dilated Cardiomyopathy (DCM) • Peripartum • Tachycardia-mediated • Sarcoidosis
Dilated Cardiomyopathy (DCM)Familial Genetic (~50%): • Family history • Genetic testing: low yield even in familial DCM (20-30%) • Promising future (?) with deep sequencing
Myocarditis Genetics Immune Response Virus Dilated Cardiomyopathy
Clinical Presentation Development of symptoms and signs of heart failure • Gradual symptoms or incidental finding • Progressive symptoms for periods varying from weeks to months with acute HF due to intercurrent illnesses • Aggressive, life-threatening fulminant heart failure (fulminant lymphocytic myocarditis, giant cell myocarditis)