Download
1 / 54
550 likes | 610 Views
Explore how the urinary system aids in maintaining homeostasis, anatomy of the kidneys, nephron functions, and the filtration process. Learn about reabsorption, secretion, and urine formation for a comprehensive understanding of renal physiology.

E N D
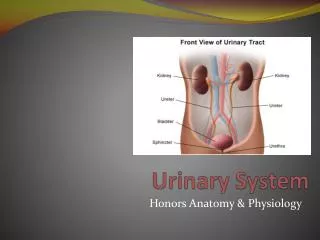
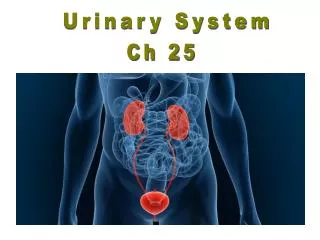
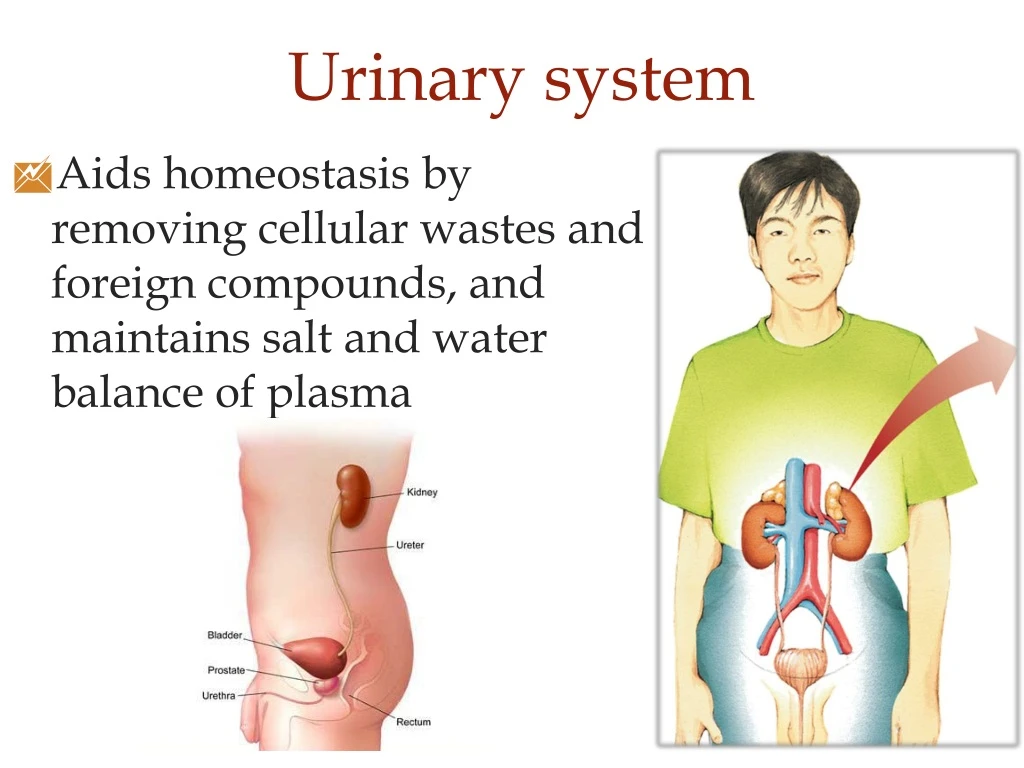
Urinary system • Aids homeostasis by removing cellular wastes and foreign compounds, and maintains salt and water balance of plasma
Kidney anatomy Renal cortex Renal medulla Cortex Renal pelvis Medulla Ureter
Nephrons Each kidney has about one million nephrons Afferent arteriole brings blood to glomerulus and then forms efferent arteriole. Efferent arteriole branches to peritubular capillaries
Let’s make the filtrate... Blood is filtered at the glomerulus. Water and solutes leave the blood and enter Bowman’s capsule.
Glomerulus physiology Bowman’s capsule contains podocytes that encircle the glomerulus. Normally blood cells and plasma proteins are not filtered
Glomerular filtration Capillary blood pressure Glomerular filtration is similar to ultrafiltration of capillaries 20% of plasma becomes filtrate 55 Osmotic pressure Hydrostatic pressure 30 15 Glomerular filtration rate (GFR) determined by: Net filtration pressure and glomerulus permeability
Adjusting GFR Blood pressure Radius of afferent arteriole Decreasing GFR helps retain fluid and salts
Filtrate is adjusted along the nephron Distal tubule Proximal tubule Cortex region Medulla region Bowman’s capsule Juxtaglomerular apparatus - helps in adjustments to filtration rate Loop of Henle
Tubular reabsorption and secretion • 180 liters per day are filtered, most is reabsorbed • Reabsorption: filtered substances leave the nephron and enter peritubular capillaries • Secretion: some substances from the peritubular capillaries enter the nephron
So what is urine, then? Everything in the nephron that does not get reabsorbed into the blood leaves as ….urine!!!
Reabsorption of Na+ (the key to it all…)
Na+reabsorption Na+ reabsorption (RA) drives the movement of many other substances in the tubule Water will “follow” Na+ movement
Page 533 Lumen Proximal tubular cell Osmosis Interstitial fluid Peritubular capillary Water channel Hydrostatic pressure Osmosis
Control of sodium RA When ECF volume is low, need to Na+ RA Na+ RA at distal and collection tubules with aldosterone. More Na+K+ pumps and Na+ channels are made Reninis the trigger for eventual release of aldosterone, along a chain of events (renin-angiotensin-aldosterone system or RAAS)
Jux.App. monitors NaCl and ECF levels Efferent arteriole Distal tubule Bowman’s capsule Bowman’s capsule Juxtaglomerular apparatus Glomerular capillaries Podocyte Distal tubule Glomerular capillaries Granular cells Juxtaglomerular apparatus Afferent arteriole
Hypertension can be due to increased renin leading to more plasma and thus high blood pressure
Glucose and amino acid reabsorption • Glucose and AA’s are cotransported w/Na+via carriers • Actively RA substances have a “tubular maximum” (when all carriers are used)
Na+ movement allows passive RA of substances. 80% of water reabsorption occurs before distal tub. by following Na+ Glucose, amino acids are reabsorbed via cotransporters If plasma levels get too high, renal threshold is reached (AAs or glucose leave in urine)
Tubular secretion H+ and K+, and organic anions are secreted to tubule • K+ secretion is driven by the Na+K+ pump
Adjusting the concentration of urine Our body tissues and filtrate are 300 mosm (osmolarity) We can make urine as dilute as 100 or concentrated as 1200 mosm Na+ gradient in renal medulla allows for control of urine osmolarity for water balance
Distal tubule Loop of Henle functions to set up high osmolarity along the collecting tubule (duct) Cortex Medulla Collecting Tubule or Duct Long loop of Henle
Collecting tubule (duct) Changing the permeability to H20 along the collecting duct controls H2O RA Vasopressin hormone controls permeability at distal and collecting tubules
Collecting duct permeability determines final amount of H2O RA 65 % of H20 RA is obligatory in the proximal tubule, 15% at Loop of Henle. 20% determined by vasopressin
Needing water Filtrate has concentration of 100 mosm/liter Cortex Medulla Collecting tubule Concentration of urine may be up to 1,200 = portions of tubule impermeable to H2O = passive diffusion of H2O = permeability to H2O increased by vasopressin * = active transport of NaCl
Too much water Filtrate has concentration of 100 mosm/liter Cortex Medulla Collecting tubule Concentration of urine may be as low as 100 = portions of tubule impermeable to H2O = passive diffusion of H2O = permeability to H2O increased by vasopressin * = active transport of NaCl
Why increased urination from alcohol? • Alcohol inhibits vasopressin • It can also temporarily reduce blood glucose (via liver effects)
Medical problems Kidney stones – caused when hard deposits form in the kidney (usually calcium, sometimes uric acid). They can enter the ureter and cause extreme pain. Urinary tract infection – 2nd most common type of infection. Bacteria introduced to urethra multiply and travel to bladder (cystitis) or further.
Things I’m assuming you know: • Know layers found throughout alimentary canal (mucosa, submucosa, muscular layers) and the term lumen • Accessory structures (pancreas, liver, salivary glands, other exocrine glands) are a part of the digestive system
Motility - propulsion and mixing Secretion of digestive enzymes, bile, mucus, water Chemical digestion Absorption Signaling What goes on during digestion…
Intrinsic nerve plexus Network of nerve fibers that controls digestive activity in gut. “Your 2nd brain”
Down the chute…oral cavity Physical digestion Mastication - mixes food with saliva Saliva - • amylase - digests starch • mucus • lysozyme Tooth decay from bacterial activity on food debris
Making saliva... Pressure and gustation promotes autonomic impulses to salivary glands • PNS and SNS signals both influence salivary glands
Bolus touches receptors in the pharynx to stimulate swallowing
Peristaltic contractions push food through the esophagus. Distention will cause a second wave and saliva release
Into the ....stomach • Storage, physical and chemical digestion • HCl • Mixing in the antrum • Bolus Chyme
Gastric emptying Pyloric sphincter Duodenum Peristaltic contraction Movement of chyme
Peristaltic contraction
Mucosa of stomach Gastric pits Mucosa Submucosa
Stomach mucosa Gastric juices! Gastric pit pH as low as 2 Mucosa cells Gastric glands Chief cells (Pepsinogen) Parietal cells (HCl)
autocatalysis Digestion Pepsinogen Pepsin Protein HCI Peptide fragments
Controlling gastric juices.. • Cephalic (“head”) phase - stimuli from the head stimulate chief and parietal cells via intrinsic plexus, gastrin released
Controlling gastric juices.. • Gastric phase – proteins, distension at stomach also stimulate gastric secretions via intrinsic plexus • Low protein, low pH is inhibitory, decreasing flow of gastric juices
Protecting the stomach from itself… • Stomach lining is protected from gastric secretions by mucus. H+ cannot enter cells • Cells are continually replaced
Stomach lining problems Peptic ulcer - stomach wall injured by acid and enzymes Injured tissue releases histamine, which stimulates acid production (…not good)
Leaving the stomach… Emptying controlled by duodenum and stomach Chyme volume promotes emptying Acid and fats in duodenum prevent gastric emptying