Download
1 / 12
260 likes | 2.1k Views
PLASMA CELL DISORDERS Plasma cells are not normally found in the peripheral blood. They account for <3.5% of the nucleated cells in the bone marrow. . The plasma cell (10-20 μm) is usually oval in shape with either a smooth or frayed outline. The N:C ratio is low.

E N D
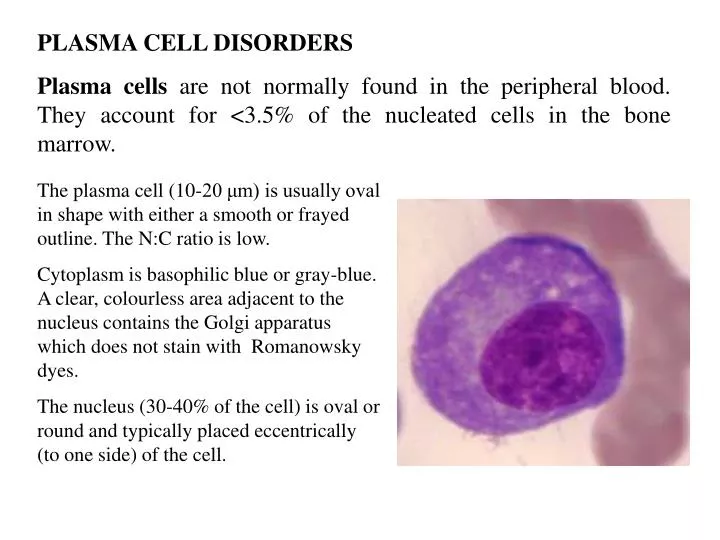
PLASMA CELL DISORDERS Plasma cells are not normally found in the peripheral blood. They account for <3.5% of the nucleated cells in the bone marrow. The plasma cell (10-20 μm) is usually oval in shape with either a smooth or frayed outline. The N:C ratio is low. Cytoplasm is basophilic blue or gray-blue. A clear, colourless area adjacent to the nucleus contains the Golgi apparatus which does not stain with Romanowsky dyes. The nucleus (30-40% of the cell) is oval or round and typically placed eccentrically (to one side) of the cell.
Russell bodies are globules (2-3 μm) of accumulated immunoglobulins in the cytoplasm of plasma cells. They vary in colour according to pH of the stain (pink or blue) or effects of alcohol fixation (colourless). Although usually round in contour these bodies may appear as rod or needle shaped crystals. Russell bodies may be found in normal bone marrow. Mott cells are plasma cells crowded with Russell bodies. An obstruction blocks the release of Golgi secretions. These cells can be found in any case of chronic plasmacytosis. Flame cells are large, multinucleated plasma cells seen in myeloma. The cytoplasm resembles a red flame.
Malignant plasma cell disorders are classified into three major groups; monoclonal gammopathy of uncertain significance (MGUS), multiple myeloma, and macroglobulinaemia. Each results from the proliferation of fully differentiated B-cells which produce monoclonal immunoglobulins (M proteins) called paraproteins. MGUS is seen in 1% of people >25 years of age, 3% in those >70 years and 10% in those >80 years. Most patients are asymptomatic and often present with the incidental finding of a paraprotein in their serum or urine. A significant number of patients progress into multiple myeloma and for this reason MGUS has been classified as a preneoplastic or malignant disorder.
Multiple myeloma is a systemic disorder. Malignant plasma cells infiltrate the BM and affect normal haemopoiesis. Osteoclast-activating factors are produced resulting in bone reabsorption. Diagnosis requires the presence of a monoclonal immunoglobulin (>3.5 g/dl of serum IgG or >2.0 g/dl of serum IgA or >1.0 g/24 hours of lambda/kappa light chains in the urine), >10% plasma cells in the bone marrow, lytic bone lesions and low levels of normal immunoglobulins. The urine contains Bence Jones protein in two-thirds of cases. BM biopsy, bone X-rays, serum and urine electrophoresis and immunoelectrophoresis are required. Rouleaux formation on the PBF correlates with a high ESR. Anaemia and thrombocytopenia may occur.
Bone fractures and bone reabsorption are major problems. Renal damage due to hypercalcaemia can lead to renal failure. Infections occur secondary to neutropenia and hypogammaglobulinaemia. Plasma cell leukaemia is a late finding in multiple myeloma (not to be confused with primary PCL). Skull X-ray in multiple myeloma showing many “punched-out” lesions.
Macroglobulinaemia (overproduction of monoclonal IgM). In Waldenstrom's macroglobulin-aemia the level of M protein is >3 g/dl. Patients present with organomegaly, hyperviscosity syndrome and anaemia. Symptoms include weight loss, fatigue and mild bleeding (usually nosebleeds). Diagnosis is made by finding plasmacytoid lymphocytes in the PBF and BM. There is an IgM M spike on serum protein electrophoresis. Hyperviscosity syndrome results from serum monoclonal IgM levels as high as 10 g/dl. Blood flow is affected resulting in neurological symptoms (blurred vision, headache and even coma). If the IgM is a cryoglobulin (precipitates in the cold) symptoms of Raynaud's phenomenon (painful extremities when exposed to cold) and thrombosis of superficial arteries can occur.
MALIGNANT LYMPHOMAS Hodgkin's and non-Hodgkin's Lymphomas. Malignant lymphomas are characterised by abnormal proliferation of lymphoid tissue (lymphocytes, histiocytes or reticulum cells). Aetiology remains uncertain but evidence would suggest infectious agents, e.g. EBV is associated with Burkitt's lymphoma of African origin. Immunodeficient patients (e.g. AIDS) also are predisposed to malignant lymphomas. Exposure to certain chemicals has also been implicated, e.g. pesticides, benzene and dioxin.
Staging is essential for prognosis and choice of treatment. Stage Extent of Disease I One lymph node region or one extralymphatic site II Two or more lymph node regions on the same side of the diaphragm III Lymph node regions on both sides of the diaphragm IV Disseminated disease involving one or more extralymphatic sites, e.g. bone marrow Malignant lymphomas have been broadly divided into Hodgkin's Disease and non-Hodgkin's lymphomas.
HODGKIN'S DISEASE A bimodal age distribution is evident; young adults and elderly adults. Pattern of spread is progressive from one lymphoid region to the next. Diagnosis Reed-Sternberg (RS) cells are diagnostic of Hodgkin's disease; large cells with two or more nuclei containing prominent central nucleoli. RS cells are derived from B-lymphocytes in lymphocyte predominant Hodgkin's and T-cells or tissue monocytes in other major subtypes.
Subtype Frequency Features Nodular sclerosis >50% Young adults, RS variants, nodules Lymphocyte predominant <10% Rare RS cells, many lymphocytes, B-lymphoid Mixed cellularity >30% More abundant RS cells Lymphocyte depleted Uncommon Numerous RS and other atypical cells Prognosis Staging is the major prognostic indicator. Patients with high-stage disease do poorly. Possible cure in early stage disease is 90% or better. 10% of survivors develop aggressive non-Hodgkin's lymphoma or AML. Radiation therapy is effective for early stage (I and II) disease but combination chemotherapy is required for higher stage disease.
Non-hodgkin's Lymphomas result from neoplastic clones of lymphocytes arising from specific stages of normal lymphoid differentiation. They are classified as low-, intermediate- or high-grade types in terms of untreated clinical behaviour: Low-grade: Diffuse small lymphocytic Follicular small cleaved cell Follicular mixed small and large cell Intermediate: Diffuse small cleaved cell Diffuse mixed small and large cell Diffuse large cell lymphoma (histiocytic) Follicular large cell lymphoma High-grade: Immunoblastic lymphoma (histiocytic) Small noncleaved cell, Burkitt-type (B-cell origin) Lymphoblastic lymphoma (tissue equivalent of ALL)
Most patients present at stage III or IV. Patients with favourable low-grade lesions may not require immediate treatment. Radiation therapy may produce durable remission. Intermediate and high-grade lesions require immediate and aggressive high-dose radiation and combination chemotherapy. Long-term survival is 50% or more. Bone marrow transplantation is being evaluated for patients who relapse.