Download
1 / 24
240 likes | 267 Views
Learn about Maryland's unique healthcare delivery system and the All-Payer Hospital Rate-Setting Model from 2014 to 2018. Discover the goals of the Total Cost of Care Model from 2019 to 2028, including the Hospital Payment Program and Care Redesign Program that aim to address population health challenges. Understand how the TCOC Model will leverage CRISP for better care coordination and outcomes, along with components such as Care Redesign Programs and alignment with non-hospital providers. Explore how the Maryland All-Payer System distributes costs equitably for sustainable healthcare.

E N D
January 22, 2019 Maryland Total Cost of Care Model: Statewide Alignment and Success Maryland Department of Health, Health Services Cost Review Commission, and Maryland Hospital Association
Agenda • Introductions • Maryland’s Unique Healthcare Delivery System • All-Payer Hospital Rate-Setting • All-Payer Model, 2014-2018 • Goals of the Total Cost of Care Model, 2019-2028 • Hospital payment program • Care Redesign Program (CRP) • Population health • Maryland Primary Care Program (MDPCP) • State Alignment and Collaboration Across Providers
Healthcare System Challenges Fragmentation & variation High costs • More Challenges Ahead. . . • Over the next decade, Maryland’s population >65 years old will increase by nearly 40% • Recent consumer polls and bipartisan focus on affordability and costs Health care disparities Coverage & Access Consumer demands Aging & sicker population
All-Payer Hospital Rate Setting andMaryland’s All-Payer Model • Since 1977, Maryland operated an all-payer, hospital rate setting system • In 2014, Maryland updated its rate setting approach through the All-Payer Model: • Patient-centered approach that focuses on improving care and outcomes • Per capita, value-based payment framework for hospitals • Stable and predictable revenues for hospitals, especially those providing rural healthcare • Provider-led efforts to reduce avoidable use and improve quality and coordination • Contractual agreement between Maryland and federal government
Value of the All-Payer System for Healthcare Consumers • Links quality and payment • Cost containment for the public • Funding for Graduate Medical Education • Transparency in hospital costs • Local access to regulators • Leverages increased federal payments • Supports state-designated health information exchange, the Chesapeake Regional Information System for our Patients (CRISP)
Public-Private Health Information Infrastructure through CRISP Supports Model • The TCOC Model will further leverage the statewide health information exchange (HIE) infrastructure through CRISP, to optimize processes, achieve the goals of the TCOC Model and improve care • CRISP reporting services to better inform patient care and population management at the point of care • Data sharing available to providers engaged in Model Programs • Available Analytic and Care Coordination Tools: • Medicare data analytics • Clinical query portal • Emergency notification services (ENS) for providers • Prescription Drug Monitoring Program (PDMP) • Ambulatory integration • Meaningful Use resources • CQM Aligned Population Health Reporting (CAliPHR)
Maryland All-Payer System Distributes Costs Equitably • With the all-payer system, hospitals are: • Paid using a common rate structure for all payers, so costs are distributed equitably • Less susceptible to margin deterioration with payer mix changes • Not dependent on volume growth • Total costs are tackled using value-based approaches and care redesign on an all-payer basis • Uncompensated care is funded equitably • Nationally, cost-shifting occurs between public and private payers Source: American Hospital Association.(1) and (2) Includes Disproportionate Share Hospital payments
Maryland Total Cost of Care (TCOC) Model • TCOC Model is designed to coordinate care for patients across hospital and non-hospital settings, improve health outcomes, and constrain the growth of costs • TCOC Model contract is a 10-year agreement (2019-2028) between Maryland and the Centers for Medicare and Medicaid Services (CMS): • 5 years (2019-2023) to build up to required Medicare TCOC savings of $300 million annually, including • Medicare Part A and Part B fee-for-service expenditures, and • Non-claims based payments • 5 years (2024-2028) to maintain Medicare TCOC savings and quality improvements • Continue to limit growth in all-payer hospital revenue per capita at 3.58% annually
Care Redesign Programs (CRP):Aligning hospitals and non-hospital providers Increase Accountability Improve Quality & Control Cost Multiple “Tracks” available to enable hospitals to redesign care and achieve quality and TCOC goals Increase accountability for high needs populations, across the spectrum of care. Alignment with Non-Hospital Providers Pathway to MACRA-tization Opportunity for hospitals to collaborate with Care Partners and make incentive payments. Pathway for a hospital’s Care Partners to participate in an advanced alternative payment model
Potential Credits for Population Health Improvement The State of Maryland and providers will jointly focus on health improvement initiatives Improved population health may offset the cost of primary care investments
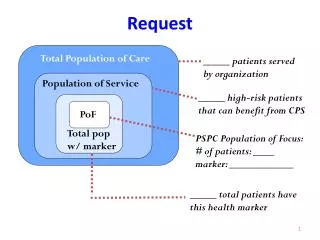
Maryland Primary Care Program (MDPCP) • As of January 1, 2019, Maryland voluntarily enrolled 380 primary care practices serving Medicare Fee For Service (FFS) beneficiaries in order to provide advanced primary care to: • Provide comprehensive care to all patients with a focus on managing the health of high- and rising-risk individuals • Provide preventive care and state-of-the-art health information technology • Address behavioral health and social needs • MDPCP strengthens and transforms primary care delivery by introducing care management and coordination supports such as: • Telemedicine, behavioral health and substance abuse counseling, care managers, and others • Care Transformation Organizations, unique to Maryland, that support small and independent practices as well as practice transformation coaches • Care Management Fees will provide resources for chronic care improvement • Aligns primary care providers with TCOC Model goals
MDPCP Benefits Patients • Freedom of choice • Team care led by my Doctor • Care Managers help smooth transitions of care • No cost sharing on enhanced services like care management • Expanded office hours • Records are available to all of my providers • Alternative, flexible care options (e.g., telemedicine, group visits, home visits) • Medication management support • Community and social support linkages (e.g., transportation, safe housing) • Behavioral health care led by my practice
Care Delivery Redesign Advanced Primary Care Functions Access & Continuity Planned Care for Health Outcomes Beneficiary & Caregiver Experience Care Management Comprehensiveness & Coordination
Hospital Perspective and Opportunities for Alignment across the Healthcare Continuum
MODEL BRINGS AMBITIOUS TARGETS Yearly Total Cost of Care Savings Targets • State’s hospitals at risk for total cost of care for 950,000 Medicare fee-for-service beneficiaries • Plus, aggressive goals: • quality improvement • health gains $162m additional savings
BIG GOALS: BETTER CARE, BETTER HEALTH Individual Health Improvement WHOLE PERSON CARE Efficiency & Affordability Accessibility & Convenience Healthy Communities
SIX KEYS TO UNLOCK VALUE Global HospitalBudgets 1 No incentive to deliver more than needed care All-Payer Hospital Rates 2 Cost burdens shared equitably by all payers Total Cost of Care Accountability 3 Hospitals each responsible for attributed lives Shared ProviderIncentives 4 Programs designed to align all care partners Population Health Goals 5 Care for communities, not just individuals Quality of CareIncentives 6 Hospitals rewarded for hitting quality targets
A SYSTEMS APPROACH IS NEEDED STATE & COMMUNITIES Better jobopportunities Strongereducation HEALTH SYSTEM Partnerships acrosscare continuum Food security Adequate &affordablehousing Robust, inclusiveworkforce Resources for modernization Family &socialsupports Integrated behavioral and physical care Safercommunities Aligned incentives Actionable healthcare management information Social connections Improvedtransportation
Katie Wunderlich, Executive Director, HSCRCHoward Haft, Executive Director, MDPCPBob Atlas, President & CEO, MHA Thank you!