Download
1 / 23
380 likes | 1.09k Views
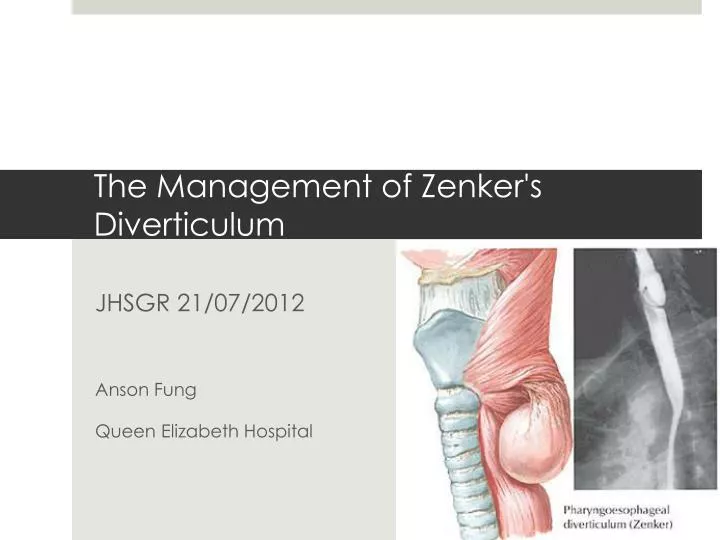
The Management of Zenker's Diverticulum. JHSGR 21/07/2012 Anson Fung Queen Elizabeth Hospital. Introduction. Zenker's diverticulum is an out- pouching of the mucosa through the Killian's triangle

E N D
The Management of Zenker's Diverticulum JHSGR 21/07/2012 Anson Fung Queen Elizabeth Hospital
Ludlow A. A case of obstructed deglutition from a preternatural dilatation of a bagformed in pharynx. Med Observations Inquiries 1767; 3:85. Introduction • Zenker's diverticulum is an out- pouching of the mucosa through the Killian's triangle • It is an area of muscular weakness between the inferior aspect of the inferior pharyngeal constrictor muscle and the cricopharyngeus muscle • The condition was first described by Ludlow in 1767 in a post- mortem examination
Zenker FA, von Ziemssen H. Krankheiten des Oesophagus. In: Handbuch der specielenPathologie und Therapie, Von Ziemssen H (Ed), FC Vogel, Leipzig 1877. p.1. Introduction • In 1877, Zenker and von Ziemssen reviewed the world literature, and since then this kind of diverticulum has been called Zenker's diverticulum
Cook IJ, GabbM, Jamieson G et al. Pharyngeal diverticulum is a disorder of upper oesophageal sphincter opening. Gastroenterology 1992; 103: 1229-35 Etiology • Secondary to the generation of high pharyngeal pressures during swallowing • Due to poor compliance of the cricopharyngeus muscle, creating a relative obstruction to the free passage of food bolus • Postulated that it involves the loss of coordination between pharyngeal contraction and the opening of the cricopharyngeus muscle
Mulder CJ, Costamagna G, Sakai P. Zenker's diverticulum: treatment using a flexible endoscope. Endoscopy 2001; 33:991. Clinical Presentation • Usually presents over the age of 60 • Majority of them being males • Asymptomatic or transient dysphagia in the early stages of the disease
Clinical Presentation • The sac will gradually grow, until it is large enough to retain mucous, food and sputum • Patient may complain of gurgling in the throat, halitosis, regurgitation, aspiration or a neck mass • Severe cachexia may present in patients with a large sac with significant esophageal obstruction and long- standing dysphagia
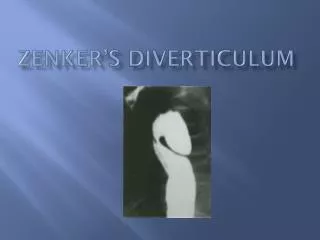
Diagnosis • Usually diagnosed with Barium studies • Diverticulum arising from the posterior wall of the esophagus • Extrinsic compression of the esophagus from behind
Diagnosis • Can present as an incidental finding in endoscopy • Tight opening of the cricopharyngeus • Lumen opening into the diverticulum
Treatment • The mainstay of treatment of symptomatic ZD has been surgery • The traditional management consisted of an open approach • Diverticular sac is amputated and myotomy of the cricopharyngeal muscle is performed
Shaw DW, Cook IJ, Jamieson GG, et al. Influence of surgery on deglutitive upper oesophageal sphincter mechanics in Zenker's diverticulum. Gut 1996; 38:806. Treatment • The efficacy of myotomy is supported by a number of surgical series in which excellent responses have been observed in 80 to 100 percent of patients • A major concern related to diverticulectomy is the potential for causing mediastinitis
Payne WS. The treatment of pharyngoesophageal diverticulum: the simple and complex. Hepatogastroenterology 1992; 39:109. Treatment • Other complications include vocal cord paralysis, pharyngocutaneous fistula, esophageal stenosis, and a recurrent or persistent Zenker’s diverticulum • The overall complication rate in one series of 900 patients treated with diverticulectomy was less than 10%
Van Overbeek JM, Hoeksemma PE. Endoscopic treatment of the hypopharyngeal diverticulum. Laryngoscope 1982:92:88-91 Treatment • Are there any minimal invasive approachs? • The concept of treating a Zenker’s diverticulum with an endoscopic approach has already been described by Mosher in 1917 • The theory is to create a common channel between the diverticulum and the esophageal lumen • This is to facilitate drainage and at the same time dividing the cricopharyngeus muscle
Ishioka S, Sakai P, Maluf- Filho F et al. Endoscopic incision of Zenker's diverticula. Endoscopy 1995; 27: 433-7 Treatment • Case reports began to emerge throughout the 1930-1950s with division of the cricopharyngeal bar with electrocautery, CO2 laser etc. • Unfortunately, many patients died of mediastinitis and a number of case series published a morbidity rate of ˜10% • Not until 1993, Collard et al. described the use of an endoscopic stapling device with a proposed advantage of shorter operative time, hospital stay and less morbidity
Treatment • The procedure is performed under general anesthesia with the neck hyperextended • A bi- valved rigid diverticuloscope is introduced into the hypopharynx with one blade is placed in the esophagus and the other in the diverticulum
Treatment • An endoscopic linear stapler is introduced under endoscopic control, with the longer jaw containing the staples and the cutting blade inserted into the esophageal introitus, then fired
B. Weksler et al. Multimedia Manual of Cardiothoracic Surgery. doi:10.1510/mmcts.2007.002923 Treatment • For anatomical reasons, trans- oral stapling is not possible in ˜3% • Patients with prominent front teeth, micrognathia, or limited neck extension will cause difficulty in placing the endoscope • Trans- oral stapling will not be possible on diverticula <2 cm in length due to inadequate access of the stapler cartridge
Narne S, Cutrone C, Bonavina L, Chella B, Peracchia A. Endoscopic diverticulotomy for the treatment of Zenker's diverticulum: results in 102 patients with staple-assisted endoscopy. Ann Otol Rhinol Laryngol 1999; 108: 810–815. Peracchia A, Bonavina L, Narne S, Segalin A, Antoniazzi L, Marotta G. Minimally invasive surgery for Zenker diverticulum: analysis of results in 95 consecutive patients. Arch Surg 1998; 133: 695–700 Treatment • There has been many successful series on endoscopic stapling and the 2 largest series comes from Italy • Endoscopic stapling was successfully completed in >95% percent of patients • Both claimed to have a response rate ˜97% • The incidence of major complications is ˜3%
Ishioka S. Endoscopic incision of Zenker's diverticula. Endoscopy 1995; 27:433-437 Treatment • What about those patients who are too frail to undergo general anesthesia? • What can we offer to the small number of patients who cannot be offered endoscopic stapling because of anatomical variations? • In 1995, Ishioka in Brazil reported his first experience with endoscopic incision of Zenker’s diverticulum using an electrosurgical system with flexible endoscopy
Treatment • The technique involves coagulation/cutting of the cricopharyngeal bar with needle knifes/ mono- polar forceps/ argon plasma coagulation • The procedure is done under sedation • A naso- gastric tube is inserted to protect the contralateral esophageal wall from thermal injury
Ishioka S. Endoscopic incision of Zenker's diverticula. Endoscopy 1995;27:433-437. Hashiba K, de Paula AL, da Silva JG, et al. Endoscopic treatment of Zenker’s diverticulum. GastrointestEndosc 1999; 49:93-97 Treatment • There have been 8 series published since 1995 on flexible endoscopic Zenker’s diverticulectomy using the needle knife • The 2 largest case series reported a response rate of ˜96% • Complication rate 5-14%
Conclusion • Zenker’s Diverticulum is a rare disease with various treatment options available • Treatment of patients with Zenker's diverticula should consider the availability of local expertise and tailor made to each patient • The advantages of endoscopic treatment are shorter operative time, hospital stay, less morbidity and easy access in case of recurrence
Cassivi SD, Deschamps C, Nichols FC, et al. Diverticula of the esophagus. SurgClin North Am 2005; 85:495-503 Conclusion • The main advantage of the flexible endoscopic approach is that it does not require general anesthesia and extension of the neck • Endoscopic treatment is not possible in diverticula <2 cm and a myotomy is all that is needed • An open surgical approach is recommended for extremely large sacs (>7cm)