Download
1 / 16
230 likes | 974 Views
Hemophilia (Royal Disease). KJFKLSDJKL. Royal Family Pedigree. Review 1. All coagulation pathways lead to activation of prothrombin and formation of fibrin clot! The activity = enzyme action Enzyme action depends on amount of protein present and the structure of protein.

E N D
Hemophilia (Royal Disease) KJFKLSDJKL
Review 1 • All coagulation pathways lead to activation of prothrombin and formation of fibrin clot! • The activity = enzyme action • Enzyme action depends on amount of protein present and the structure of protein Graphic accessed http://www.ganfyd.org/images/3/32/CoagulationAndFibrolyticPathways.png, 2009.
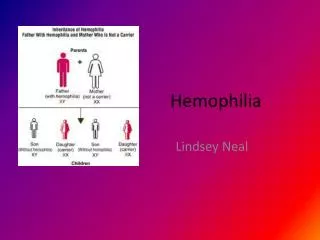
Introduction :Genetics and InheritanceX-linked Recessive • X-linked genes are never passed from father to son • An affected female must have an affected father • Males are always hemizygous for X linked traits, that is, they can never be heterozygoses or homozygotes • Males are never carriers • In a male a single dose of a mutant gene will produce a mutant phenotype in the male • In a female will be either homozygous for the normal gene, heterozygous (carrier), or homozygous (have trait) for the mutant gene. Information and graphic accessed http://www.ncbi.nlm.nih.gov/bookshelf/br.fcgi?book=gene&part=glossary&rendertype=box&id=further_illus-226, 2009.
Hemophilias Introduction • Hemophilia • Inherited • X-linked (recessive) • A & B • Autosomal • C • Single factor deficiencies • Anatomic soft tissue bleeding Graphic accessed URL http://www.daviddarling.info/images/hemophilia_inheritance_1.gif, 2008.
Hemophilias Introduction: Genetics A & B genes for both FVIII and FIX are located on the long arm of chromosome X The gene for FVIII (F8C) is unusually large FVIII contains 2332 amino acids Approximately 40% of cases of severe FVIII deficiency arise from a large inversion that disrupts the FVIII gene. Deletions, insertions, and point mutations account for the remaining 50-60% of hemophilia A defects The FIX gene (F9) is small FIX contains 415 amino acids Point mutations and deletions in the FIX gene are the most common causes of hemophilia B C gene for factor XI is on the distal arm of chromosome 4 Mutations described so far are associated with mainly failed or reduced production of the active protein, and only a few are related to the production of a dysfunctional molecule. Graphic accessed http://www.biochem.arizona.edu/classes/bioc471/pages/Lecture25/TktR-2.jpeg, 2009.
Hemophilias Introduction • Prevalence • North America & Europe • A - 1 in 5000 male births • US 21 cases per 100,000 male individuals w/ 60% severe disease • B – 1 in 25,000 male births • US 5.3 cases per 100,000 male individuals w/ 44% severe disease • C – 1 in 100,000 population • High prevalence in Ashkenzai and Iraqi Jews • Israel – 8% rate • United Kingdom 383 in 58 million population • Severity Classification • Clinical bleeding symptoms Or • Plasma procoagulant levels • < 1% normal factor activity • Severe • 1 – 5% normal factor activity • Moderately severe • 5 – 40% normal factor activity • Mild hemophilia
Classic Hemophilia – VIII Deficiency • FVIII 2-chain glycoprotein produced by liver and endothelium • Cleaved by thrombin producing a calcium dependent heterodimer that complexes with IXa • VIIIa-IXa (Tenase) cleaves X • Deficiency of VIII slows production of thrombin • hemorrhage Graphic accessed http://kuwaitmd.hsc.edu.kw/main/files/images/Coagulation_cascade.png, 2009.
Hemophilia A: Clinical Manifestations • Anatomic Bleeds • Deep muscle • Joint • Wound oozing • CNS bleeds – can be the fatal event in those younger than 18 years of age • Body cavity hemorrhage • Loss of mobility • Neurological symptoms http://www.kelleycom.com/blog/uploaded_images/synovitis-784213.jpg Graphic accessed URL http://library.thinkquest.org/05aug/00112/Images/knee.jpg, 2008.
Hemophilia A Diagnosis • Clinical Presentation • Family history • Abnormal neonatal bleeding • Umbilicus • Circumcision • Intracranial • Laboratory • Prolonged PTT • PT prolonged in newborns • Factor assay • VIII, IX, XI • Rule out: • vWD • PLT disorders • Other factor deficiencies • Hypo/dysfibrinogenenia Graphic accessed URL http://labtestsonline.org/understanding/analytes/coag_cascade/Coag%20Testing%20Cascade.pdf, 2008.
Products available Recombinant FVIII Factor VIII concentrate Recombinant VIIa DDAVP – increase vWF Aminocaproic acid – anti-fibrinolytic FVIII 1 U/kg increases FVIII plasma levels by 2%. The reaction half-time is 8-12 hours. Treatment regimen examples Severe epistaxis Factor concentrate until 50% level achieved Also consider aminocaproic acid 1-2 days Surgery Factor VII concentrate until 80% level achieved 10-14 days Treatment • Goal – reduce morbidity, prevent complications
Hemophilia B a.k.a Christmas Disease • X-linked, recessive disorder • Factor IX deficiency, dysfunctional factor IX, or factor IX inhibitors • spontaneous hemorrhage • excessive hemorrhage in response to trauma • Occurrence • 1 in 25,000 males in US • 1 in 60,000 males worldwide Graphic accessed URL http://coursewareobjects.elsevier.com/objects/elr/Rodak3e/IC/jpg/Chapter41/041005.jpg, 2008.
Lab Studies CBC PLT count – NL PT - NL PTT - prolonged Factor XI - severe disease less than 1%; moderate disease 1-5%; mild disease greater than 5%. Hemophilia B – Differential Diagnosis • Hemophilia A • VWDVitamin K and other factor deficiencies • Afibrinogenemia • Fibrinolytic diseases • Platelet disorders
Treatment Recombinant factor IX - level should be corrected to 100% of normal for potentially serious hemorrhage Goal to keep trough level > 50% activity Coagulation factor IX concentrates - used to correct the patient's native deficiency Goals: 1) achieve a normal hematologic response to hemorrhage; 2) prevent hemorrhage Factor IX complex concentrates (II, X, VII) Circumvent inhibitor issue FFP Coagulation Factor VIIa (Recombinant) - activate coagulation factor X to factor Xa as well as coagulation factor IX to IXa Epsilon aminocaproic acid (Amicar)
Hemophilia C • Factor XI deficiency (variable bleeding usually following trauma/surgical interventions) • Autosomal inheritance • 1 per 100,000 persons • Even heterozygotes can have bleeds • Mild to moderate bleeding • bleeding risk in hemophilia C is not always influenced by the severity of the deficiency • Prevalence in Ashkenzai Jews • Severity of bleeding episode not correlated with factor levels • PT, TT – normal • PTT – prolonged • Rule out • PLT dysfunction • Other factor deficiencies
Hemophilia C Treatment • “Factor XI concentrates • FFP • Fibrin glue (e.g., Tisseel VH) • Aminocaproic acid Matthew Prasad, MB, BS, DCH - Director, Hemostasis and Hematology Program, Professor of Pediatrics, University of New Mexico.