Download
1 / 64
640 likes | 794 Views
The Development, Implementation, and Assessment of a Culturally Innovative HIV/AIDS Intervention for Hispanic Drug Injectors. Antonio L. Estrada, Ph.D., MSPH Director Mexican American Studies & Research Center And Professor Mel & Enid Zuckerman Arizona College of Public Health

E N D
The Development, Implementation, and Assessment of a Culturally Innovative HIV/AIDS Intervention for Hispanic Drug Injectors Antonio L. Estrada, Ph.D., MSPH Director Mexican American Studies & Research Center And Professor Mel & Enid Zuckerman Arizona College of Public Health The University of Arizona 9th Annual Summer Public Health Videoconference on Minority Health June 12, 2003 Support for this research was provided by the National Institute on Drug Abuse, Grant # R01-DA10162, National Institutes of Health
Background • In 2000, the rate of AIDS cases among Hispanic males was more than 3 times the rate found among non-Hispanic white males (47.2 per 100,000 vs. 14.0 per 100,000). • Moreover, the rate of AIDS cases among Hispanic females was more than 6 times the rate found among non-Hispanic white females (13.8 per 100,000 vs. 2.2 per 100,000).
Background • The transmission mode of injecting drug use (IDU) has shown a dramatic increase in AIDS cases from 1990-2000. During the last decade, IDU increased by over 400 percent. • For Hispanic males, injecting drug use as a transmission mode increased by a factor of 7. • For Hispanic females, injecting drug use and sex with an injecting drug user as transmission modes increased by a factor of 8.
Background • Hispanics, as well as African Americans, tend to have higher case-fatality rates from AIDS than non-Hispanic whites due to a lack of health care access, early detection, and treatment costs. • Increasing disparity is seen in the percent of those infected with HIV; 42% among Non-Hispanic Whites compared to 58% among minorities (CDC, 2001).
Background • Previous studies have shown that AIDS rates among Hispanics vary markedly depending on the specific Hispanic sub-group examined (e.g., Mexican American, Puerto Rican, Central/South American, Cuban, etc.).
Adult/adolescent AIDS cases among Hispanics, by exposure category and place of birth, reported in 2000, United States 1. Excludes persons born in U.S. dependencies, possessions, and independent nations in free association with the United States. Ancestry data for U.S.-born Hispanics are not collected. 2. Includes 234 Hispanics born in locations other than those listed, and 1,193 Hispanics whose place of birth is unknown.3. See Technical Notes.
Male Hispanic AIDS Cases by Exposure Category Reported through December 2001, U.S. Note: Cases are for adults and adolescents Source: Center for Disease Control, HIV/AIDS Surveillance Report, December 2001
Female Hispanic AIDS Cases by Exposure Category Reported through December 2001, U.S. Note: Cases are for adults and adolescents Source: Center for Disease Control, HIV/AIDS Surveillance Report, December 2001
Pediatric Hispanic AIDS Cases by Exposure Category Reported through December 2001, U.S. Source: Center for Disease Control, HIV/AIDS Surveillance Report, December 2001
HIV/AIDS Risk Behaviors Injection-Related/Syringe-Mediated Risk Behaviors • Frequency of injection • Type of drug injected (Cocaine, Methamphetamine, Heroin) • Common drug purchases (pooling money) • Multi-person reuse of needle/syringe • Lack of appropriate bleaching of needle/syringe • Sharing the cooker, cotton, rinse water • Front-loading (syringe mediated drug dispersal) • Back-loading (syringe mediated drug dispersal)
HIV/AIDS Risk Behaviors Sexually Related Risk Behaviors • Sexual relations under the influence of drugs/alcohol • Exchanging sex for money or drugs • Sexual bingeing • Unprotected sex with an HIV+ individual • Unprotected sex with an HIV+ IDU • Hierarchy of risk in sexual relations (oral, vaginal, anal)
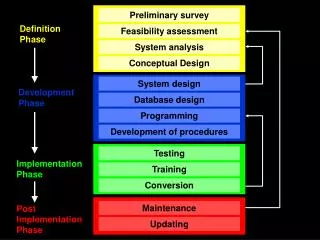
Methods for Chronic Disease Prevention and Control (Public Health Model) Secondary prevention Tertiary prevention Prevention strategy Primary prevention Asymptomatic Symptomatic Population’s disease status Susceptible Reduced prevalence/ consequence Reduced complications/ disability Effects Reduced disease incidence
Four Major Theoretical Models Used in HIV/AIDS Prevention I.The Health Belief Model (Becker) • Relevant health motivation and knowledge (importance of health) • Vulnerability to disease • Disease perceived as threatening • Efficacy and feasibility of behavior change • Cues to action • Barriers to action
Four Major Theoretical Models Used in HIV/AIDS Prevention (contd.) II. Social Cognitive Theory (Bandura) • Observation and modeling of behaviors in a social group • Normative behaviors that are valued/endorsed • Perceived Self-efficacy • Social network influences • Role models
Four Major Theoretical Models Used in HIV/AIDS Prevention (contd.) • III. Theory of Reasoned Action/Planned Behavior • (Fishbein and Ajzen) • Behavioral intentions • Subjective norms • Behavioral and normative beliefs • Attitudes toward behaviors • Perceived behavioral control
Four Major Theoretical Models Used in HIV/AIDS Prevention (contd.) • IV. Transtheoretical Model (Stages of Change) • (Prochaska and DiClemente) • Pre-contemplative • Contemplative • Ready for action • Action • Maintenance • Relapse
NIMH Theorists WorkshopConsensus on Eight Areas 1. BehavioralIntentions 2. Environmental Constraints 3. Ability (skills) 4. Anticipated Outcomes or Attitudes 5. Normative Influences 6. Self-standards 7. Emotion (positive or negative attitudes toward behavior change) 8. Perceived Self-efficacy
Designing and Implementing a Culturally Innovative Intervention
Cultural Sensitivity Versus Cultural Competency Cultural Sensitivity • Translation of materials into Spanish • Hiring of bilingual/bicultural staff • Delivering the intervention within the targeted community (community-based) • Recognizing cultural differences • Creating a culturally appropriate environment • All of the above
Cultural Sensitivity Versus Cultural Competency Cultural Competency Similar to cultural sensitivity, but differs by building the overall intervention on cultural concepts, normative/cultural beliefs, or the essence of the culture itself
Defining Culturally Appropriate Interventions Marin, G. (1993): Culturally Appropriate Interventions • Based on the cultural values of the group • Strategies that comprise the intervention reflect the subjective culture (attitudes, expectations, norms) of the group • The components that make up the strategies reflect the behavioral preferences and expectations of the group members
Defining Culturally Appropriate Interventions Singer, (1991): Various forms/approaches for interventions • “Culturally sensitive” approaches attempt to be socioculturally empathetic, in that they recognize the importance of training staff to be cognizant of racial/ethnic issues and sensitivities
Defining Culturally Appropriate Interventions • In addition to the above, “culturally appropriate” approaches also incorporate a specific awareness of the cultural and linguistic patterns of the target community. To help people feel “at home” and to build a rapport quickly.
Defining Culturally Appropriate Interventions • “Culturally innovative” approaches incorporate features of the other types but in addition struggle to consciously mobilize and enhance cultural beliefs, symbols, concepts, values and roles as core elements of the intervention process. They intentionally attempt to find ways to “use culture” therapeutically to both reach participants and to assist them in making behavioral changes.
Defining Culturally Appropriate Interventions • “Socioculturally congruent” approaches, while including elements of the other approaches, are especially concerned with establishing congruence between program work and community efforts in the struggle for self-determination and self-development. The ultimate goal is to assist participants to view their culture as an empowerment tool.
Hispanic Cultural Concepts That Were Identified for Possible Use to Derive the “Culturally Innovative” Intervention Acculturation: The degree to which Mexican Americans are more “traditional” in their orientation to Hispanic or Anglo culture. La Vida Loca: The lifestyle characteristics of Mexican American injection drug users. Familism: The significance of family to the individual. Simpatia: The smooth/non-confrontational context of social interactions. Personalismo: The preference for relationships with same-ethnic members in a social group.
Hispanic Cultural Concepts That Were Identified for Possible Use to Derive the “Culturally Innovative” Intervention Machismo: Machismo of the streets vs. Machismo of the home. Respeto: The need to maintain one’s personal integrity and that of others. Controlarse: The degree of self-control an individual has over certain behaviors and feelings. Confianza: The establishment of a trusting, safe and open bond between two people. Traditionalism:The degree to which one adheres to traditional beliefs and customs (e.g., gender roles).
Deriving and Validating Cultural and Subcultural Concepts Elicitation Research: • Used this approach to identify and define cultural concepts with Hispanic IDUs • Forty in-depth interviews and four focus groups with Hispanic IDUs were conducted in the first year of the study • Several cultural and subcultural concepts were identified
Deriving and Validating Cultural and Subcultural Concepts Machismo: • For me being macho means always having drugs. • Being macho is an important part of who I am. • A woman should give in to her husband in almost all matters. • It is a man’s right to drink and use drugs if he wants to. • For me, being macho is controlling my drug use.
Deriving and Validating Cultural and Subcultural Concepts • It is macho to get high on any drug available. • Drug use makes my friends think I am macho. • It is macho to have lots of money and drugs. • To be macho you can never let your guard down. • To be macho is not to be addicted. • Those who sell drugs are macho.
Deriving and Validating Cultural and Subcultural Concepts Religiosity: • I am a very religious person. • Healing comes only from God. • My faith in God has guided my life and helped me through personal crises I have had. • I go to church regularly.
Deriving and Validating Cultural and Subcultural Concepts • I want my children to have a religious background. • Good health and happiness happens to people who obey God’s commandments. • I have a lot of faith in the power of God. • I pray every day.
Deriving and Validating Cultural and Subcultural Concepts Familism: • More parents should teach their children to be loyal to the family. • I rely on my family for help when I need it. • No matter what the cost, dealing with my relatives’ problems comes first.
Deriving and Validating Cultural and Subcultural Concepts • It is important to me to be respected by my family. • In spite of my drug use, I always try to take care of my family. • My family is very important to me.
Deriving and Validating Cultural and Subcultural Concepts • Traditionalism: • I prefer to live in a small town where everyone knows each other. • Husbands and wives should share equally in child rearing and child care. • It is hard to meet and get to know people in large cities.
Deriving and Validating Cultural and Subcultural Concepts • You should know your family history so you can pass it along to your children. • Adult children should visit their parents regularly. • We should make time for friends and others.
Deriving and Validating Cultural and Subcultural Concepts • Children should be taught to always be close to their families. • We are in such a hurry sometimes that we forget to enjoy life. • When making important decisions in my life, I like to consult members of my family. • Tradition and ritual serve to remind us of the rich history of our institutions and our society.
One to One Intervention Guidelines Theoretical Model • Eclectic, primarily derived from the Theory of Reasoned Action/Planned Behavior, Cognitive Social Theory, and the Health Belief Model. The intervention model is similar to the AIDS Risk Reduction Model (ARRM), in that it has several stages - labeling, salience, commitment, action, and maintenance. The model was guided by an empowerment philosophy using a case management approach.
Stages, Influences, Assessments and Interventions for HIV/AIDS Risk Management
One to One Intervention Guidelines Psychosocial and Behavioral Measures: • Perceived Risk of HIV/AIDS; • Facilitators and Inhibitors to taking preventive action; • HIV/AIDS knowledge; • HIV/AIDS risk behaviors (injection and sexual); • Normative influences; • Perceived Self-efficacy; • Response Efficacy (perceived benefits of behavior change); • Behavioral Intentions to perform preventive behaviors