Download
1 / 18
190 likes | 414 Views
Laryngeal Cancer. Clerk 2: 吳柏宣 陳昱潔 Supervisor: 李家和醫師. Anatomy. Anatomy. Vaezi, MF . Nature Clinical Practice Gastroenterology & Hepatology (2005) 2 , 595-603. Anatomy– Supraglottic larynx. It consists of epiglottis, false vocal cords, ventricles, aryepiglottic folds, and arytenoids.

E N D
Laryngeal Cancer Clerk 2: 吳柏宣 陳昱潔Supervisor: 李家和醫師
Anatomy Vaezi, MF . Nature Clinical Practice Gastroenterology & Hepatology (2005) 2, 595-603
Anatomy– Supraglottic larynx • It consists of epiglottis, false vocal cords, ventricles, aryepiglottic folds, and arytenoids
Anatomy– Glottic larynx • It consists of the true vocal cords and anterior commissure and posterior commissure
Anatomy– Subglottic larynx • It consists of the region between the vocal cords and the trachea.
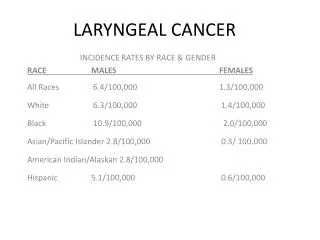
Epidemiology • Male : Female = 4 : 1 • Age: 50~60 y/o • > 90% squamous cell cancer • 位置分類 • Glottic cancer80% • Supraglottic cancer20% • Subglottic cancer1%
Risk Factors Smoking(最主要危險因子)。 Alcohol(有加成作用)。 HPV type16 and 18 GERD。 長期暴露於石棉、芥子氣 、石化氣體
Clinical Presentation • Mass effect: hoarseness, dysphagia, hemoptysis, neck mass, airway compromise (difficulty breathing), aspiration • Throat pain, ear pain (referred through CN X branch) • Suggests advanced stage • Hoarseness = allow for early detection of glottic cancer • Weight loss
Clinical Presentation – cont’ • Physical Exam • Complete head and neck exam • Palpation for nodes; restricted laryngeal crepitus. • Quality of voice • Breathy voice = cord paralysis • Muffled voice = supraglottic lesion • Laryngoscopy • Stroboscopic video laryngoscopy
Staging • Glottis • Tis: CA in-situ • T1: limited to cord; • T1a: one cord; T1b: two cords • T2: extends to supraglottis, and/or subglottis, and/or w/impaired cord mobility • T3: limited to larynx w/vocal cord fixation and/or invades paraglottic space, and/or minor thyroid cartilage erosion • T4a: invades thyroid cartilage and/or tissues beyond larynx • T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures • Subglottis • T1: limited to subglottis • T2: extends to vocal cord with normal or impaired mobility • T3: limited to larynx w/vocal cord fixation • T4a: invades cricoid or thyroid cartilage, and/or invades tissues beyond the larynx • T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures • Supraglottis • T1: limited to subsite of supraglots w/normal cord mobility • T2: invade mucosa of > 1 subsite of supraglottis, glottis, or outside of supraglottis w/out fixation of the larynx • T3: limited to larynx w/vocal cord fixation and/or invades postcricoid area, pre-epiglottic tissues, paraglottic space, and/or minor thyroid cartilage erosion • T4a: invades thyroid cartilage and/or tissues beyond larynx • T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures
Staging • Subglottis • Tis: CA in-situ • T1: limited to subglottis • T2: extends to vocal cord with normal or impaired mobility • T3: limited to larynx w/vocal cord fixation • T4a: invades cricoid or thyroid cartilage, and/or invades tissues beyond the larynx • T4b: invades prevertebral space, encases carotid artery, or invades mediastinal structures • Nodes • N0: no regional node mets • N1: single ipsilateral node, ≤ 3 cm • N2a: single ipsilateral node, > 3 cm, ≤ 6 cm • N2b: multiple ipsilateral nodes, ≤ 6 cm • N2c: bilateral or contralateral nodes, ≤ 6 cm • N3: node > 6 cm • Mets • Mx: unknown • M0: no distant mets • M1: distant mets
Stage Grouping Early stage Advanced stage
Treatment – Early Stage (I/II) • Early stage (T1 and T2) can be treated with radiotherapy or surgery (endoscopic resection or open organ-preservation surgery) alone, both offer the 85-95% cure rate. • Surgery has a shorter treatment period, saves radiation for recurrence, but may have worse voice outcomes • Radiotherapy is given for 6-7 weeks, avoids surgical risks but has own complications
Treatment – Early stage (I/II) • XRT complications include: • Mucositis • Odynophagia • Laryngeal edema • Xerostomia • Stricture and fibrosis • Radionecrosis • Hypothyroidism
Treatment – Advanced Stage (III/IV) • Advanced stage lesions often receive surgery with adjuvant radiation • Most T3 and T4 lesions require a total laryngectomy • Some small T3 and lesser sized tumors can be treated with partial larygectomy
Treatment – Advanced Stage (III/IV) • Chemotherapy can be used in addition to irradiation in advanced stage cancers • Two agents used are Cisplatinum and 5-flourouracil (5-FU) • Cisplatin thought to sensitize cancer cells to XRT enhancing its effectiveness when used concurrently.
Treatment – Advanced Stage (III/IV) • Modified or radical neck dissections are indicated in the presence of nodal disease • Neck dissections may be performed in patients with supra or subglottic T2 tumors even in the absence of nodal disease • N0 necks can have a selective dissection sparing the SCM, IJ, and XI • N1 necks usually have a modified dissection of levels II-IV