Download
1 / 64
640 likes | 800 Views
Celine Bicquart Advanced Laryngeal Cancers. October 19, 2006. Overview of Talk. Case Presentation Anatomy and Lymph Node Drainage of the Larynx Overview of Laryngeal Epidemiology Staging of Patient Review of Literature Patient Treatment Plan. DS. ID: 49 y/o male

E N D
Celine BicquartAdvanced Laryngeal Cancers October 19, 2006
Overview of Talk • Case Presentation • Anatomy and Lymph Node Drainage of the Larynx • Overview of Laryngeal Epidemiology • Staging of Patient • Review of Literature • Patient Treatment Plan
DS • ID: 49 y/o male • HPI: Hoarse since January 2006 with odynophagia and dysphagia. 10 lb wt loss in August. • Referred to ENT at OHSU. • 8/16/06- CT neck- 17 x 14mm enhancing soft tissue lesion filling L piriform sinus. Involves L. supraglottis, L glottis, L subglottis with midline focal area of destruction of thyroid cartilage. +Posterior L level III adenopathy.
HPI cont’d • FNA of L neck node- Metastatic poorly- differentiated SqCCa with high N:C ratio. • 9/15/06- Total larynectomy, L neck dissection II-IV, L hemithyroidectomy, Pec major flap. Path: 4.3cm G3 Invasive Squamous Cell, negative margins. Invades through thyroid cartilage, but thyroid gland uninvolved. 4/14 Level II. +ECE. 2/6 Level III. –ECE. 1/8 Level IV. –ECE. +perineural invasion. Indeterminate angiolymphatic space invasion.
PMH: Seizures • Meds: Dilantin 300mg qd, Oxycodone q3-5h, Nicotine patch 21mg qd • Allergies: NKDA • PSH: Laryngectomy • SH: Single. Lives in Portland. Receives disability, previously did odd jobs. Smoked 1.5ppd x 30y. Cut back in 05/06. Now uses nicotine patch. Drinks 1-2 drinks qd. • PE: Healing incisions of left neck dissection and pec major flap. Stoma appears patent. No fistula noted. No discharge from stoma noted.
Supraglottis- high incidence of LN metastasis: jugulodigastric, jugulocarotid, juguloomohyoid. Glottis- Subglottis- 1 ant: mid and lower jugular to prelaryngeal node ???? 2 post: paratracheal
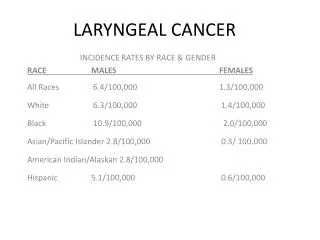
12000 new cases yearly- 2% of all cancers60-65% glottic30-35% supraglottic5% subglotticM:Fp53-mutated in 47% smokers
Signs and Symptoms • Hoarseness- MC presenting sx of glottic ca • Sore throat- MC presenting sx of supra ca • Odynophagia- MC presenting sx of supra ca • Foreign Body Sensation • Dysphagia • Stridor • Pain • Hemoptysis • Otalgia- via vagus and nerve of Arnold. • Weight loss • Airway obstruction Risk Factors: -Tobacco -Alcohol
Evaluation and Work-up • Complete H&P • Assess for adenopathy in neck. • Loss of Thyroid click: sign of post-cricoid extension. • Mass over thyroid signifies thyroid cartilage invasion.
Indirect mirror exam for visualization. “EEEeeeeee.” • Fiberoptic flexible laryngoscopy. • CXR for metastatic evaluation • CBC, LFTs. If abnormal, may get CT abd, bone scan.
CT, MRI • Performed before bx. • MRI is better to delineate soft-tissue extent of primary tumor. • CT is better for evaluating bone invasion. • CT also very useful for detecting subclinical LN metastasis. • Want to look for pre-epiglottic, periglottic space invasion, subglottic and extralaryngeal extension, and cartilage invasion.
Direct laryngoscopy with bx for tissue dx, disease extent. • Usually performed as part of panendoscopy to r/u multiple tumors.
Squamous Cell Carcinoma of the Larynx 95% SqCCa. TVC- well to mod-diff Supra and subglottis- more poorly diff
Following surgery, DS has had a slow recovery. FT still in place secondary to residual swelling. Patient reports dysphagia. • Patient also reports dyspnea on exertion.
Clinical Question My patient’s cancer was a T4, for which the standard of care had been a total laryngectomy followed by adjuvant radiation. • TL results in disease control rates of 70-80%; and with TE punctures for voice restoration, patients can eventually regain their verbal communication skills. • In light of this good disease control rate, is there a way to obtain equivalent survival while sacrificing less quality of life?
Looked at induction chemo + definitive RT vs. conventional TL + PORT • Stratified according to KPS, Stage III vs. IV, Nodes, tumor site Patients with no response or locally recurrent disease underwent salvage laryngectomy.
VA Trial • After two cycles of chemotherapy: CR 31% and PR 54%. (Overall response 85%) • At median f/u of 33 months, the estimated 2-year survival was 68 percent (95% CI, 60 to 76%) for both tx groups (P = 0.9846)
VA Trial • Toxicity due to RT was similar in both arms. • Grade 2 mucositis slightly higher in chemo group 38% vs. 24% in TL group. • Higher incidence of surgical complications in salvage cases after RT vs. just after chemo.
VA Trial • Patterns of recurrence differed significantly between the two groups, with more local recurrences (P = 0.0005) and fewer distant metastases (P = 0.016) in the chemotherapy group than in the surgery group.
A total of 59 patients in the chemotherapy group (36 percent) required total laryngectomy. • So….64% preserved their larynx without compromising OS. • Induction chemo does enhance the effectiveness of RT, but since no direct comparison was made between chemoRT vs. RT alone, the role of chemo remains uncertain.
Determine if chemo followed by XRT was comparable with standard surgery +PORT in pts with T2-4, N0-2b SCCA of the pyriform sinus or AE fold • Multi-centered, prospective, randomized trial • PR or CR assessed after each cycle. If after any cycle, no response, went directly to surgery. Only CR went on to XRT
EORTC Trial • 97/100 pts. started chemo as randomized. • 60/97 proceeded to complete chemo + RT. (70Gy, 65Gy) • 8/97 required surgical salvage. (55Gy, 60Gy) • 92/94 pts. had surgery as randomized. • 89/92 had post-op RT. (60Gy) • Chemotherapy complete responders were more frequent among those with T2 disease (82%) than those with T3 (48%) or T4 (0%) disease.
Disease Free SurvivalCI: 0.52-1.43 • Overall survival chemo (57%)>surgery (43%) at 3 years but equal at 5 years. NB- small number of pts. at 5y. CI: 0.50- 1.48
No difference in locoregional failure. • Increase in distant mets in surgery group (36%) compared to (25%) in chemo arm. p<.041 • Survival with functional larynx with no LR, tracheostomy, FT, gastrostomy at 3 and 5 years = 28% and 17% respectively. • Rate of functional larynx in those who died of causes other than local disease progression and died with a functional larynx at 3 and 5 years= 42% and 35% respectively. • EORTC study: conclusions • Induction chemo is safe for hypopharyngeal cancer. • Fewer distant mets and increased time until mets appear • CR: T2 (82%) > T3 (48%) > T4 (0%)
Conclusions so far… • Organ preservation is possible • Role of induction chemo is still not exactly known. • Distant metastases decreased, and time to DM increased. • EORTC trial had small number of patients. • Lower larynx preservation rates in the EORTC was a result of more stringent selection criteria.
Determine role of induction chemo vs concurrent chemo vs radiation alone in laryngeal preservation for pts with stage 3 and 4 SqCCa of the larynx • T1 and high-volume T4 tumors where excluded (>1cm into tongue base or penetrating cartilage invasion) • Multi-center, prospective, randomized
-cisplatin 100mg/m2; 5-FU 1000mg/m2-For concurrent: cisplatin given on day 1,22,43 of RT-RT to primary: 70Gy in 35 @2Gy-RT to neck, supraclav, post. neck: 50Gy-Salvage RT for those who failed induction chemo was 50-70Gy-Questionnaires were filled out at baseline and at each f/u.
Induction Chemo Arm • 168/174 patients received induction chemo. • 144 had either a CR (21%) or PR (64%), allowing them to receive PORT. • 24/168 patients who could not go onto RT. Only 7 went directly to RL. • 11/24 received chemo/RT, and all had CR, and of these, only 1 needed TL. • At end of RT: 150/174 (86%) had CR.
Concurrent ChemoRT arm • 120/172 (70%) received all 3 doses cisplatin. • 40/172 (23%)received 2 doses. • At end of RT: 154/172 (90%) had CR. RT alone arm • At end of RT: 148/172 (86%) had CR.
2 and 5 year overall survival did not differ • 76% vs 74% vs 75% at 2 years • 55% vs 54% vs 56% at 5 years Disease Free Survival
Concurrent resulted in significantly fewer LRs compared to both induction chemo and RT alone. Concurrent vs Induction p<.02. Concurrent vs. RT alone p<.001 No statistical difference between induction and RT alone arms.
Effect on Distant Metastases Chemo reduced the rate of DMs. The only statistically significant difference was between the concurrent vs. RT alone arm. p<.03
Laryngeal Preservation at 3.8y IMPORTANT!! Induction chemotherapy followed by RT when compared to RT alone, did not significantly improve the rate of laryngeal preservation.
Conclusion from RTOG 91-11 • Concurrent chemoRT is superior to both induction chemo and RT alone in regards to locoregional control, laryngeal preservation, and distant metastases. • Induction chemo showed benefits in only improving DFS, and decreasing rate of DMs. No effect on LR or OS. • Overall survival does not differ significantly between treatment arms. (76% at 2y) • Concurrent chemo does cause twice as severe mucosal effects, potentially contributing to delayed recovery of swallowing in this group.
Is laryngeal preservation (LP) with induction chemotherapy (ICT) safe in the treatment of hypopharyngeal SCC? Final results of the phase III EORTC 24891 trial.Journal of Clinical Oncology, 2004 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 22, No 14S (July 15 Supplement), 2004: 5531 • Ultimate disease control, including successful salvage after XRT, was not significantly different between both arms. • As of 12/2003, 14 % of pts in arm 1 and 17 % of pts in arm 2 were still alive. The hypopharynx SCC evolution was the cause of death in 43 pts in arm 1 and in 41 pts in arm 2. • In arm 2 survival with a functional larynx in place was 22 % at 5y and 9 % at 10y. • Conclusions: this final analysis has confirmed the preliminary results with similar survival curves as compared with conventional treatment and allowed 2/3 of the survivors to retain their larynx.
Additional therapies • Molecular targets have been identified which may hold promise in the treatment of H&N SqCCa. • Overexpression of EGFR is recognized in more than 95% of SqCCas. The EGFR and its ligands, EGF and TFG alpha are important in cell proliferation, adhesion, invasion and angiogenesis. • Administration of the EGFR monoclonal antibody (cetuximab) has been shown to increase radiosensitization, decrease tumor cell line growth and increase apoptosis. • Other novel chemotherapeutics include agents to inhibit tyrosine kinase, angiogenesis inhibitors, and agents that have selective toxicity to hypoxic cells.
Function and Quality of Life • Preserving the larynx is great, but not as great if the larynx is not effective. • How well does it function after concurrent chemoRT? • How do patients feel about their ability to communicate and swallow?
Long-term Quality of Life After Treatment of Laryngeal Cancer Jeffrey E. Terrell, MD; Susan G. Fisher, PhD; Gregory T. Wolf, MD; for the Veterans Affairs Laryngeal Cancer Study GroupArch Otolaryngol Head Neck Surg. 1998;124:964-971. • 1998 follow up: 46/65 surviving pts, 71% RR • 25 surgery+PORT, 21 experimental arm • HNQOL, SF-36 General Health Measure Short Form, Beck Depression Inventory, alcohol and smoking surveys.
Quality of Life f/u of VA Study • Those with larynx fared significantly better from the standpoint of speech communication. • At 2 years post-treatment, patients with successful organ preservation had regained their pretx level of functioning for 2/3 measures tested (intelligibility and reading rate) and exceeded pretx performance on the 3rd (a communication profile used to assess general communication status). • TL + PORT pts had a decrease in all 3 speech communication-related measures despite availability of all modes of speech rehabilitation and therapy. • Measures of swallowing dysfunction were similar between both arms.
Quality of Life f/u to VA study Pts with successful organ preservation: • had better scores on all domains of the SF-36 compared to those who underwent TL. • scored significantly better on the bodily pain and mental health domain of the SF-36. • scored significantly better on the emotion domain and their impression of their response to treatment on the HNQOL survey. At long-term f/u, 10 of 45 patients had BDI scores consistent with moderate or severe depression. • 9 of those 10 had undergone TL.
Conclusions from VA Study • Better QOL in the CT+RT appears to be related to more freedom from pain, better emotional well being, and lower levels of depression than to preservation of speech function
RTOG91-11 Speech Percentages of speech impairment at 1 and 2y. • No difference among 3 groups in regard to speech at 12 or 24m. Moderate speech impairment: difficulty in pronouncing some words and being understood on the telephone.
RTOG 91-11-Laryngeal Function @1y • No difference in groups’ QOL • 2-yr all three groups similar with 16%, 15%, 14% reporting difficulty swallowing
Grade and frequency of toxic acute effects was similar in the induction and RT alone arms: mostly grade 3 in-field effects on skin and mucous membranes. Concurrent chemoRT had chemo-related toxic acute effects (neutropenia, severe N/V, increased rates of severe radiation-related mucosal, pharyngeal and esophageal effects. Rates of late toxic effects were similar among groups.
Patients who are treated with larynx-preserving modalities are still at risk of having to undergo salvage laryngectomy in the future. • In these patients, is there any added morbidity associated with salvage laryngectomy?
Danish Society for Head and Neck Oncology (2003) • Wanted to look at surgical outcome of 472 pts with salvage laryngectomy after XRT from 1987-1997 • Specific outcome looked at was development of pharyngocutaneous fistula. • 89 fistulas lasting > 2 weeks; Overall fistula rate = 19% • Number of TLs per year decreased linearly (from 58 to 37), whereas the annual number of fistulae increased slightly (from 7 to 11). • RR in 1987 =12% • RR in 1997 =30% • Grau C, Johansen LV, Hansen HS, Andersen E, Godballe C, Andersen LJ, Hald J, Moller H, Overgaard M, Bastholt L, Greisen O, Harbo G, Hansen O, Overgaard J. Salvage Laryngectomy and Pharyngocutaneous Fistulae after Primary Radiotherapy for Head and Neck Cancer: a National Survey From DAHANCA. Head and Neck. Sep 2003. 25:711-716.