Download
1 / 31
310 likes | 651 Views
LEUKEMIA. ↑ leukocytes Acute leukemias 1. Acute Lymphoblastic Leukemia (ALL) 2. Acute Myelogenous Leukemia (AML). Chronic leukemias 1.Chronic L ymphoblastic Leukemia (CLL) 2. Chronic Myelogenous Leukemia (CML). Leukemias. Acute Leukemias. Blast predominate Child or elder

E N D
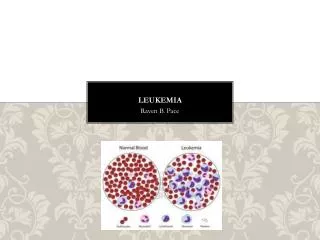
↑ leukocytes Acute leukemias 1. Acute Lymphoblastic Leukemia (ALL) 2. Acute Myelogenous Leukemia (AML) Chronic leukemias 1.Chronic Lymphoblastic Leukemia (CLL) 2. Chronic Myelogenous Leukemia (CML) Leukemias
Acute Leukemias • Blast predominate • Child or elder • Short & drastic course • ALL – Lymphoblasts (pre-B or pre-T) • AML – Myeloblasts
Chronic Leukemias • More mature cells • Middle age • Longer & less devastating course • CLL – Lymphocytes • CML – Myeloid stem cells
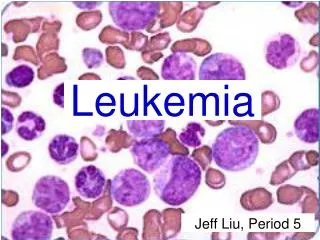
Acute Leukemias • accumulation of blasts in the marrow
Acute Lymphoblastic Leukemia (ALL) • Children • Lymphoblasts (pre-B or pre-T) • Neoplastic transformation of the lymphoid stem cells • Progressive accumulation of Lymphoblasts in the bone marrow • Suppression of normal hemopoiesis
• Primarily a disease of children and young adults • B-cell subtype (80%) • T-cell subtype (20%)
ALL Abrupt onset Signs and symptoms related to: • Suppression of normal hemopoiesis bone pain and tenderness • Tissue infiltration ( megaly) (lymph nodes, spleen, liver, testicles, CNS) • Mediastinal mass ( T-ALL ) thymus involvement Headache, vomiting, nerve palsies from meningeal spread.
Signs &Symptoms • Anemia • Infection • Bleeding • Bone pain • Arthritis • Splenomegaly • Lymphadenopathy • CNS involvement
ALL - PROGNOSIS Favorable: Unfavorable: Pre-B T or mature B Age 3-7 < 1, > 10 WBC < 10 000/uL > 50 000/uL Female Male Minimal organ Prominent organ involvement involvement
ALL Prognosis: • Age 3-7, pre-B, > 90% - CR( 2/3 - cure ) • Adults, mature B and T-ALL: Less favorable Therapy: Chemotherapy supportive care, BMT
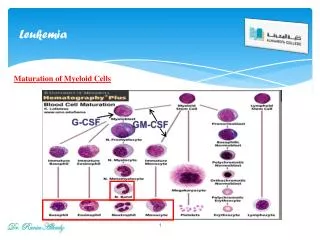
ACUTEMYELOGENOUS LEUKEMIA ( AML ) • Adults • Myeloblasts • monoblasts, eosinoblasts, megakarioblasts, proerythroblasts, basophiloblasts • Auer rods in the cytoplasm of the cells • Very rapidly progressive malignancy
Differentiation from ALL may be made by microscopy – presence of Auer Rods. • Can also be made based on immunotyping and molecular methods. Clinical features based on • Marrow failure –anemia, bleeding, DIC, infection… • Leukemic infiltration – bone pain, CNS signs, hepatosplenomegaly, lymphadenopathy… • Constitutional upset -- malaise, fever, weakness, polyarthritis.
Course: • Rapidly fatal if untreated (< 2 mo ) • Median survival - 3 years after chem.. • Adverse prognostic factors: Age > 60 Previous chemotherapy Leukocytosis > 100,000 /ul Therapy:Chemotherapy, supportive, BMT
***Remember this*** For Acute leukemias • acute leukemias = too many blasts in the marrow • 2 broad categories: AML vs. ALL • a hematologic urgency • prognosis is poor in adults; but good in kids with ALL.
CHRONIC LYMPHOCYTIC LEUKEMIA (CLL) A monoclonal lymphoproliferative disorder characterized by lymphocytosis(>4000/cu.mm), lymphadenopathy and splenomegaly B - CLL > 95% T - CLL
CLL •Most common adult leukemia in Western society (30% of all leukemias) • Monoclonal proliferation of the small lymphocytes… • Age > 40 M:F / 2:1
CLL - Pathology Blood: • Lymphocytosis ( > 10,000 u/L - diagnostic ) • (+) Coombs test (20%) • Hypogammaglobulinemia (50-70%) • Anemia, thrombocytopenia, neutropenia Bone marrow: • nodular / interstitial infiltrates • diffuse - obliteration of normal hemopoiesis Lymphadenopathy,Hepatosplenomegaly(50-60%)
CLL - Clinical course Initially: asymptomatic Advanced disease: • bacterial infections, hemorrhage Prognostic factors: • extent of tumor burden • pattern of marrow infiltration • chromosomal abnormalities Median survival: ~ 6 years
CLL - Course • CONVERSION TO PROLYMPHOCYTIC LEUKEMIA (10%) • RICHTER SYNDROME (5%)(AGGRESSIVE LYMPHOMA) • DEATH OFTEN DUE TO INFECTIONS..
CLL • One more peripheral blood findings in CLL is Presence of Smudge cells ( parachute cells). • Along with increased number of normal appearing lymphocytes.
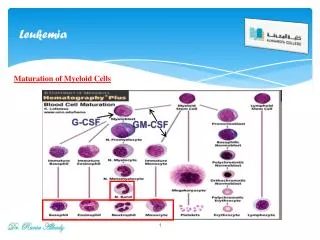
mainly uncontrolled proliferation of myeloid cells. • Males more than females • Splenomegaly – sometimes massive..
**Philadelphia chromosome** • Hybrid chromosome with translocation between the long arm of chr. 9 and long arm of chr.22 . --- t(9:22). • May be present in granulocyte, RBC or platelet precursors in more than 95% of CML.. • Absence of these chr. may have worse prognosis.
CML - Clinical Features 15 - 20% of all leukemias; age 25-60 Symptoms: - non-specific - related to hypermetabolism (high cell turnover) - related to splenomegaly Course: - chronic phase (mean survival, 3-4y) - accelerated phase - blast crisis / myeloid or lymphoid (survival, < 1y) Therapy: chemotherapy; BMT
CML: Sustained granulocytosis with immature cells; low LAP score; bone marrow pathology; Philadelphia chromosome • LAP – leukocyte alkaline phosphatase