Download
1 / 26
270 likes | 579 Views
Anatomy and Physiology of the Respiratory System and Nursing Diagnosis of Chronic Broncitis. Function of Respiratory System. Gas Exchange a. External respiration b. Internal respiration c. Cellular respiration Ventilation Blood Reservoir Systemic Blood Filter Fluid Exchange

E N D
Anatomy and Physiology of the Respiratory Systemand Nursing Diagnosis of Chronic Broncitis
Function of Respiratory System • Gas Exchange a. External respiration b. Internal respiration c. Cellular respiration • Ventilation • Blood Reservoir • Systemic Blood Filter • Fluid Exchange • Metabolic Functions of the Lungs
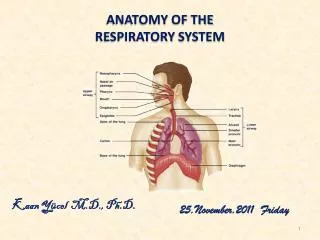
Upper Airway • Nose • Paranasal sinuses • Oral cavity • Pharynx
Nose The nose humidifies and warms air to body temperature and filters inspired air by trapping particles >6μm in diameter. • Paranasal sinuses Posterior sphenoid sinuses that provide temperature insulation and voice resonance enhancement. • Oral cavity Involved in digestion, speech, and respiration. • Pharynx It separates inspired air from food and water. a. Nasopharynx b. Oropharynx c. Laryngopharynx d. Pharyngeal musculature
Lower Airway • Larynx • Trachea • Bronchi • Lungs
1. Larynx Lies between the upper and lower airway at the level of C4-6. 2. Trachea a flexibel, slightly rigid tubular organ. • Bronchi • Enter the lungs at the hilus • Right bronchus: wider, shorter and straighter than left • Bronchi subdivide into smaller tubes. • Lungs • Left lung Two lobes • Right lung three lobes
Mechanics of Breathing • Inspiration The active process of contracting the diaphragm downward to create a negative pressure within the thoracic cavity that draws gas into the lungs. a. Diaphragm b. External intercostal muscles c. Abdominal muscles d. Neck muscles (scalene and sternocleidomastoid)
B. Expiration The passive act of relaxing the respiratory muscles allowing a decrease in thoracic size and the elastic recoil of the lungs to deflate the lungs. a. Intercostal and accessory muscles b. Abdominal muscles
PHATOPHYSIOLOGY Mucus hypersecretion : incresed size and number of submucous glands in the large bronchi. The increase of mucous leads to airway narrowing and airway obstruction In smaller airway, chronic inflammation leads to repeated cycles of injury and repair of airways and therefor scar tissue formation and narrowing airways. Reduction of alveolar ventilation due to increased secretions. Expiratory airflow limitation Breathlessness due to airway narrowing and bronchoconstriction
TOKSIK DISFUNGTION SILIA INFLAMASI HIPERSEKRESI REFLEKS VAGAL INFEKSI INCREASE BRONCHIAL SECRETION INCREASE BRONKOMOTOR TONE CHRONICAL BRONCITIS
CLASIFICATION and TYPE • Simple Chronic Bronchitis, characterized by coughing and other minor complaints. • Chronicbronchitis Mucopurulen,characterized by thick phlegm cough, purulent (yellowish). • Chronic bronchitis with airway constriction, characterized by coughing up phlegm that is accompanied by severe shortness of breath and wheezing sound.
Etiology 1. Cigarette Smoking hiperpaplasia of mukusbrochi gland and metaplasia of silia activity inhibition, alveolarmakrofag, surfaktan depreciation of force expiration volume 2. Infection Virus infection secondary bacteria infection (HaemophilusinfluenzaedanStreptococuspneumonia) infection on upper respiratory infection on lower respiratory 3. Polution Industrial polution (fiber, gas, cement) but it have not big influence
4. Breed • Deficiencies of alpha-1 anti tripsin abnormal preolitikenzyme tissue damage • 5. Social-Economy Factor • Low environment and economy • 6. Old age • Increasing age decreasing imunity susceptible disease
Clinical Appreance Symptoms of Chronic Bronchitis may include : • Much phlegm or voluminous cough • Sometimes making purulen sputum or blood cough • Dispnea • A moment dispnea on sleep dispneaon cold air and misty progresif on activity or rest. Sometimes espoused tired right heart. • Listened wheezing
Describing bronchi stricture • Listened gargling on inspiration • Describing phlegm • Breast pain • Fever • Headache
Diagnostic Assesment • History • Exposure to risk factor • Past medical history (ex: asma) • Family history of COPD • Chronic Cough: lenght of time • Smoking history • Respiratory illness
Potensial Abnormal Physical Exam • Assesment of severity based on level of symptoms • Severity of spirometric abnormalities • Characteristic of respiratory pattern • Breath sounds • Shortness of breath with speech • Sputum producing color
C. Laboratorium Diagnostic • Chest X-ray • Postbronchodilator • Pulmonary function test • Arterial blood gasses • Oxygen saturation
Nursing Diagnosis • Ineffective airway clearance related to bronchospasm, increased production of secret. SD:- The client complained of cough with shortness of breathOD: - The client looks coughing up phlegm • Pain disorder a sense of comfort with respect to the presence of pleural inflammation, characterized by: SD : Clientcomplains of chest pain centerOD: Client winced in pain
Disruption of intolerance activity with respect to the physical weakness, characterized by: SD : clients say easily tired, lethargic body when many brgerakOD: Clients seem weak, so that helped a client's activities such as sitting, eating and to the bathroom • Disorders of bed rest with respect to the presence of cough DS: Clients complain: insomniaDO: sclera appear red, the frequency of sleep ± 5 hours / day
Nursing Intervention • Vital sign observation Rasional: to checked vital sign’s changes • Teach a client for effective coughing exercises Rasional: effective coughing exercises can help the client remove secretion • Assessthe level of pain with a pain scale Rasional: to determine the quality of perceived pain intensity • Helpclients meet the daily needs Rasional: By helping clients to mobilize bit by bit, the client can perform activities independently without the help of.
The Therapy • Airway clearance techniques: Controlled cough and deep breathing, flutter valve, Thairpy vest, PEP theraphy • Glucocorticosteroids: regular treatment does not modify long term decline of FEV1 but they are apropiate for symtomatic COPD patient with FEV1<50% • Hydration: to keep secretions thin and minimal 6-8 glasses of water/ day
Nutrition: maintain physical condition with increased fats and decreased carbohydrat in order to decrease CO2 production. • Antibiotics: used when secretions become infected. • Patient teaching: Relaxation techniques, cough control, and pursed lip breathing.
Thanks for your nice attention
http://www.getbodysmart.com/ap/respiratorysystem/menu/menu.htmlhttp://www.getbodysmart.com/ap/respiratorysystem/menu/menu.html