Download
1 / 31
320 likes | 327 Views
Learn how implementing team training and checklists can enhance communication, change culture, and improve surgical outcomes in a hospital setting with data-driven results.

E N D
ACS NSQIP 30 Day Outcomes Supports Implementation of a Surgical Checklist Changing Culture Scott Ellner, DO, MPH, FACS Cynthia Ross-Richardson, MS, BSN, RN, CNOR Saint Francis Hospital and Medical Center University of Connecticut Integrated Surgery Residency May 21, 2012
Objectives • Discuss the use of a validated safety attitudes questionnaire to understand behavior in the surgical environment • Discuss OR team training to change culture • Discuss the implementation and use of the AORN surgical checklist • Discuss the use of the American College of Surgeons National Surgical Quality Improvement Program to assess 30-day postoperative complications
Demographics • 600 Bed tertiary care facility • Level 2 Trauma Center • UConn Surgical Residency • 8,000 General surgery cases/yr. • 30 Operating rooms ACS NSQIP since 2007 ACS TQIP since 2011 SFHMC Hartford, Connecticut
Operating Room Team Circa 1914
Operating Room Team Circa 2012
Evidence-based Risk-adjusted Data driven = Improved Surgical Outcomes American College of SurgeonsNational Surgical Quality Improvement Program Shukri F. Khuri, MD
30-Day Adverse Event Rate 3,314 General Surgery Cases Collected by 2010
Post-Operative Urinary Tract Infections Observed Rate: 2.41% Expected Rate: 1.47% O/E Ratio: 1.64 Status:Needs Improvement 2009
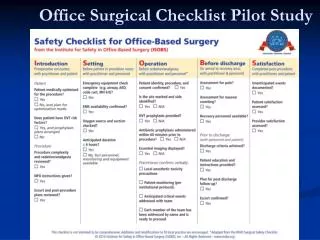
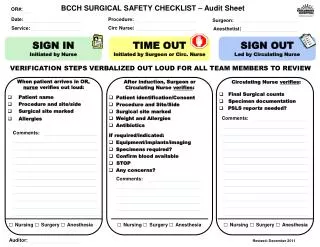
Patient Safety Project • Implementation and compliance with AORN (WHO) checklist • Pilot project 75 general surgery cases compared to historical controls to reduce post-operative 30-day complications as measured by NSQIP • Team Training Sessions to Change Culture
Metrics/Outcomes • Reduce NSQIP 30 day post-operative outcomes • Urinary Tract Infection • Surgical Site Infection • Hospital Acquired Pneumonia • Thromboembolic events • Transfusion rate • No Retained Foreign Bodies • Assess Safety Attitudes – Likert Scale • Circulating Nurse Exits • Compliance with AORN Checklist • Qualitative Observations
Identifying Culture Communication Behavior Rituals Tolerance
SAQ Participants N=161
Pre-Training Observations of Team Communication • Language Barriers • Shared commitment • Assumptions • Efficiency • Interruptions • Side conversation • Multi-tasking • Complacency • Personal Issues • Workload/Staff fluctuation • Fatigue and stress • Disruptive behavior
Why Team Training? • Enhances communication • Addresses improper behavior • Helps to build trust • Gives all employees a voice • Improves the overall safety culture • Encourages leadership
Team Training Tool • Session 1 – Crucial Conversations • Session 2 – Getting What You Want: Communication Strategies That Help You Get What You Need • Session 3 – When the Going Gets Tough: Achieving a Positive Outcome
Launch of Team Training Violence Safety Safety Pool of Shared Meaning Safety Silence
Barriers • Complacency • Resistance • Exposing failures • Challenging years of • embedded culture • Compliance • Training • Uneasy Leadership
OR Change Agents • OR Ambassadors • OR Observers • Executive Leadership
Observed Qualitative Results Good Teamwork. Specimen sent to Pathology with follow-up during case Joking by surgeon at expense of female personnel No equipment malfunctions. Staff in room joined together to announce Time-Out and Debrief CRNA brought open cup of Coffee, raised sheet to cover view of anesthesia area Anesthesia initiating the Time-Out Patient paged overhead by surgical floor while in surgery No site marked for hernia. Circulator recognized and asked surgeon to mark.
Quantitative Results N= 75 general surgery cases
Post-Operative Urinary Tract Infections Observed Rate: 1.23% Expected Rate: 1.43% O/E Ratio: 0.86 Status: As Expected 2009 2011
Post-Operative Pneumonia Observed Rate: 0.65% Expected Rate: 1.24% O/E Ratio: 0.52 Status: Exemplary 2009 2011
Circulating Nurse Exits • Average 9 exits (4 hour case)* • Observed range 0-25 exits (average 3 exits) • Checklist Compliance 97% • Increase in the number of OR exits led to higher rates of patient morbidity *Christian et al. Surgery 2006
Take Home Points • Acknowledge the need for change • Measure baseline attitudes – SAQ • Implement team training curriculum • Observe and audit checklist utilization • Recognize and address barriers • Provide resources for sustainability • Identify metrics to demonstrate change