Download
1 / 28
320 likes | 826 Views
Leukemia. Rita All Carrie Warner. Definition. Leukemia is a group of malignant diseases that result in changes to circulating lymphocytes characterized by diffuse, abnormal growth of leukocytic precursors in the marrow.

E N D
Leukemia Rita All Carrie Warner
Definition • Leukemia is a group of malignant diseases that result in changes to circulating lymphocytes characterized by diffuse, abnormal growth of leukocytic precursors in the marrow. • The uncontrolled increase in immature white blood cells suppresses normal hematopoietic stem cells leading to anemia and thrombocytopenia. • Causes life threatening infections due to ineffective WBC function. • Classification is made by the course of the illness and types of cells and tissues involved. • Staging is not possible as it is already circulating. (Burns, 2013; Larson, 2014).
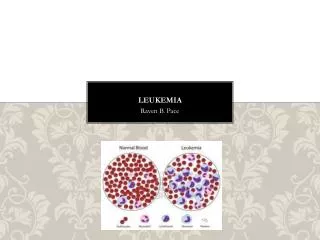
Normal blood versus leukemia blood (American Cancer Society, 2014)
Leukemia Vs. Lymphoma • According to the American Joint Committee on Cancer (AJCC) • Circulating cells= leukemia • Tumor masses in lymph nodes and tissues= lymphoma • If both= lymphoma/leukemia • Emerging research suggests these are the same diseases in different stages • Chronic lymphocytic leukemia= small lymphocytic lymphoma (a form of non-Hodgkins lymphoma) • If greater than 25% of marrow replaced by cancerous lymphocytes, it is usually considered leukemia. • Also if the lymph nodes are very large, diagnosis will generally be lymphoma. (American Cancer Society, 2014)
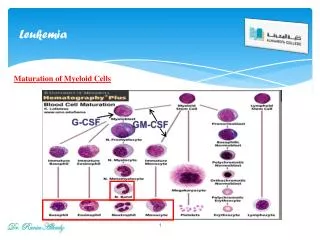
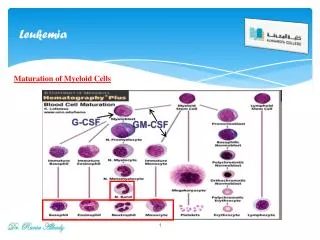
Pathophysiology • Normal bone marrow elements are replaced with blast cells that are abnormal and poorly differentiated. • The abnormal cells (Lymphoblasts or Myeloid cells) take over and cause unregulated clonal proliferation of malignant cells, crowding out other healthy cell groups. • Chronic lymphocytic leukemia progresses slowly and can last decades. • People with Chronic Myeloid leukemia acquired a chromosomal abnormality that causes part of one chromosome to break off and join another, the short chromosome called the Philadelphia chromosome, which produces an enzyme that causes WBCs to grow out of control, that can ultimately result in acute leukemia. (Larson, 2014)
Genesis of blood cells (National Cancer Institute, 2013)
Etiology • Unknown etiology for all types, but higher incidences with some that have: • Infection • Radiation • Chemical and Drug exposure • Epstein- Barr may play a role in in Burkitt leukemia/ lymphoma. • Genetic mutations may lead to disruption of lymphocytes and prolonged survival. (Domino, 2014; Burns, 2013; National Cancer Institute, 2013).
Incidence • There were 48,610 new cases of leukemia in 2013, 2.9% of all cancer cases. • There were 23,720 deaths in 2013 from leukemia, 4.1% of all cancer deaths. • The five year survival rate for leukemia is 56% • Leukemia is the most common form of childhood cancer, 41% of pediatric malignancies in children less than 15 (Burns, 2013). • Four main types of leukemias, with many rare varants and subtypes. • ALL- In the US- 1,000 adult cases per year, median age 35-40 years old, incidence increases with age, males slightly more prevalent than females. Accounts for 80% of all childhood leukemia cases, peak age 2-6 years old. Occurs one out of every 29,000 children annually (Burns, 2013). • AML- Increases with age, median age 70 years. 13,500 cases in 2007, second most common type of leukemia for adults and children. Affects males slightly more than females. • CLL- 15,000 to 17,000 new cases reported annually. Most common form of leukemia in adults. Median age of diagnosis is 70 years, with rising incidence in those greater than 55 years old. Males have higher incidence 1.7:1, and higher with Caucasian than African Americans. • CML- 1.6 cases per 100,000 annually. Greatest in 50-60 year olds, with males having higher incidence 1.3:1. Accounts for 15-20 % of adult leukemias • (Burns, 2013; Domino, 2014)
Leukemias (Lee, 2009)
Screening • There is no individual screening test for Leukemias. • Those with risk factors can be monitored more diligently with routine exams and labs. • Routine or illness physical: Presence of organomegaly- hepatosplenomegaly , enlarged lymph nodes. • CBC with Differential (Often found during routine exam or illness) • Low or high white blood cells, varying levels of neutropenia • Thrombocytopenia present in 85 % of cases • Peripheral smear- malignant cells • Low hemoglobin, less than 9.0 • Liver Function Tests may show elevations (Burns, 2013)
Risk Factors • ALL- Less than 15 years old, greater than 60 years old. Chemical exposure to benzene or radiation. Can follow aplastic anemia. • AML- Genetic predisposition (Down’s syndrome, Bloom’s syndrome), Fanconi anemia, neurofibromatosis, Li- Fraumeni Syndrome, Wiskott- Aldrich syndrome, Kostmann syndrome, and Diamond- blackfan anemia. Radiation exposure, Immunodeficiency states, Chemical and drug exposure (nitrogen mustard, benzene), Myelodysplastic syndromes, Cigarette smoking (20%). • CLL- Mostly uncertain risk factors, possible chronic immune stimulation. • CML- Ionizing radiation exposure • All leukemias: possibly other causes such as workplace exposures from organic solvents, pesticides, herbicides, hair dyes; electromagnetic fields, birth weight over 7.7 lbs, mom over 35 yrs at birth, and parent exposures. (Domino, 2014).
Clinical Findings Children: • Signs and symptoms related to leukemic replacement of bone marrow/ absence of blood cell precursors • Anemia, Pallor, listlessness • Irritability, chronically tired • History of repeated infections, fever, weight loss • Bleeding- epistaxis, petechiae, hematomas • Lymphadenopathy and hepatosplenomegaly • Bone and joint pain • CNS symptoms if brain involvement • Abnormal CBC, low or high white cell count with out of proportion differential • Testicular pain (Burns, 2013) Adults: • Acute forms have bone and joint pain • Gingival hyperplasia with bleeding • S/S infection- Fevers, chills, palpitations, shortness of breath • Skin eruptions, easy bruising, prolonged bleeding times • Chronic forms c/o fatigue, night sweats, low grade fevers • CML- leukostasis- blurred vision, respiratory distress, priapism • Organomegaly with chronic form, hepatosplenomegaly with enlarged spleen and lymph nodes, assoc with N/V • Pallor, Anemia • Abnormal CBC, low or high white cell count with out of proportion differential (Dunphy, 2011)
Differential Diagnosis Acute Lymphocytic Leukemia • AML • CML in Lymphoid blast phase • Prolymphocytic leukemia • Malignant Lymphomas • Multiple Myeloma • Bone marrow metastases from solid tumors (breast, prostate, lung, renal) • Myelodysplastic syndromes • Aplastic anemia • Myelofibrosis • Autoimmune disease (lupus, felty syndrome) • Infectious mononucleosis • Pertussis • Autoimmune Thrombocytopenia purpura • Leukemoid reaction to infection (Domino, 2014). Acute Myeloid Leukemia • Virus Induced Cytopenia, lymphadenopathy, and organomegaly • Immune Cytopenias (including Systemic lupus erythmatosis) • Drug induced cytopenias • Other marrow failure and infiltrative disease (aplastic anemia, paroxysmal nocturnal hemoglobinuria, myelodysplastic syndromes, Gaucher disease) (Domino, 2014).
Differential Diagnosis Chronic Myelogenous Leukemia • Chronic Myelomonocytic leukemia • Chronic neutrophilic leukemia • Chronic eosinophilic leukemia • Juvenile myelomonocytic leukemia • Infectious mononucleosis • Leukemoid reaction • Polycythemiavera • Treatment with granulocyte stimulating factors • Acute myelogenous leukemia • Acute lymphoblastic leukemia • Atypical CML (Domino, 2014). Chronic Lymphocytic Leukemia • Bacterial Tuberculosis • Infectious mononucleosis • Non hodgkins Lymphoma • Hairy cell leukemia • Waldenstrommacroglobulinemia • Large granular lymphocytic leukemia (Domino, 2014).
Social/ Environmental Considerations • For children: • No physical activities • Limited exposure to other children and family members due to risk of contracting infection. • Frequent hospitalizations for treatments, and follow ups. • Frequent illness due to disease and treatment modalities. • Changing of physical self, loss of hair, swelling, pale skin and dark circles under eyes, weight loss, central lines or ports. • Limited exposure to animals. • Family pressures with medical bills and transportation. • Threat of mortality. • For adults: • Frequent monitoring, hospitalizations for testing, treatments, and follow up. • Missed work, or need for leave of absence. • Loss of income due to missed work time, leave of absence, and elevated medical bills. • Family dynamic changes, the primary caregiver may become the one being cared for. • Changing of physical self, loss of hair, swelling, pale skin and dark circles under eyes, weight loss, central lines or ports. • Family pressures due to decreased income, increased bills, changes in family dynamics, and feeling of lack of self worth. • Threat of mortality. (Dunphy, 2011; Larson, 2014)
Laboratory tests/ diagnostics • CBC with Manual Differential • Low or high white blood cells, varying levels of neutropenia • Thrombocytopenia present in 85 % of cases • Peripheral smear- malignant cells • Low hemoglobin, less than 9.0 • Uric acid level • Can be elevated or high • LDH • Elevated • PCR (polymerase chain reaction) • Presence of biomarkers in blood/ bone marrow cells . DNA abnormality marker with AML or CML “philadelphia chromosome” • Liver Function Tests • Elevation due to inflammation of liver • Sed Rate • Elevation • CRP • Elevation • Bone marrow Bx/ aspiration • Replacement of normal marrow cells by blast cells • Should parallel peripheral smear • Lumbar Puncture, CXR, CT scans, MRIs- to rule out other pathology, CNS involvement, hepatosplenomegaly (Burns, 2013)
Management/ Treatment Guidelines • Treatment varies on • Type of leukemia • If chronic, usually asymptomatic, immediate treatment may not be required • Goal is for regular checkups, control disease and symptoms, and is seldom curable. • If acute, treatment begins right away • Goal is Remission, prevention of relapse, and it can be curable. • Extent of disease • If has been treated for cancer before • Age, symptoms, general health Maintaining health physically and mentally (National Cancer Institute, 2013).
Management/ Treatment Guidelines • Bone marrow transplant • Splenectomy • Radiation • Clinical trials • Nutritional support (IV fluids/ hyperalimentation) • Avoidance of antiplatelets (ASA) • Neutropenic guidelines/ reverse isolation for infection prevention • Blood transfusions (Domino, 2014)
Treatment guidelines • AML- Intermediate and high risk patients curative potential only from Bone marrow transplant. • Transretinoic acid and arsenic trioxide promote maturation to granulocytes. • Idarubicin is used for induction therapy in 3-4 cycles. • CLL- Most patients do not require active treatment. • Early treatment is not advised. • High risk patients are only treated. • Three main groups of drugs: (COP or CHOP treatment- cyclophosphamide, vincristine, prednisone, doxorubicin) • 1. Alkylating agents- chlorambusil, bendamustine, cyclophosphamide • 2. Purine analogues- fludarabine, pentostatin • 3. Monoclonal antibodies- rituximab, alemtuzumab • CML- Bone marrow transplant is the only known cure. TKI’s (imatinib) provide long term control of disease, no immature blood cells, and no Philadelpha positive metaphases. • (Katzung, Masters, & Trevor, 2012). • ALL- 4 phases of treatment • Remission induction chemotherapy • One month • Kill as many cancer causing cells as possible • Corticosteroids • Transfusions • goal- Induce remission • Consolidation, or CNS prophylaxis • Preventative therapy • Stops spread to brain/ spinal cord • High Dose IV or Intrathecal chemo • Radiation to the brain PRN • Usually lasts 2-6 months • Intensification therapy • Starts when in remission • high dose chemo to kill any lingering cells1-2 times, 1-2 months each time • Maintenance therapy • Chemo for several years to remain in remission • Girls- 2 years, Boys- 3 years
Leukemia pharmacology • Chemotherapeutics- common toxic side effects include nausea, vomiting, immuno and myelosuppression. Can also cause hepato , nephro, and neurotoxicity. They are often used in multiples. • Alkylating agents- DNA synthesis and function inhibition, as well as mitosis inhibition and catastrophe, leading to cell death. (bendamustine, Cyclophosphamide, Busulfan) • Antimetabolites- Inhibit DNA synthesis and repair (Cytarabine, Fludarabine, Cladribine, 6-MP, 6- Thioguanine, methotrexate) • Antitumor antibiotics- oxygen free radicals bind to DNA and RNA breaking it and interfering with replication. (Daunorubicin, Idarubicin) • Asparginase- enzyme isolated from E coli, hydrolyzes L asparagine, causing rapid inhibition of protein synthesis. • Imatinib- Inhibits tyrosine kinase in Philadephia chromosome related CML. Corticosteriods- used in conjunction with Chemotherapeutics to decrease inflammation, immunosuppression, and further chances for remission. (Katzung, Masters, & Trevor, 2012).
Complications • Infection • Anemia • Excess bleeding/ bruising (low PLT) • Clotting disorders ( elevated PLT), DVT, CVA • Richter transformation- 3-5% of patients with CLL develop diffuse large B cell lymphoma, and prognosis is generally poor. • Other cancer developments due to cancer or treatments- Kaposi Sarcoma, Melanoma, Bladder, Lung, stomach, throat cancers. • Hairy cell leukemia- can develop hodgkins, non- hodgkins, thyroid ca. • Kidney failure (Rare) • Ruptured spleen (due to enlargement) • CNS involvement- seizures, headache, vomiting, confusion, loss of coordination • Depression • Pain (increased WBC in marrow) • Infertility • Death • Therapy related illness, including avascular necrosis, transfusion reaction, neurotoxicity, tumor lysis syndrome, • Late effects (66%)- learning disabilities, poor work performance, psyche distress, health insurance discrimination, “chemo brain”- inability to concentrate. (Dunphy, 2011; Burns, 2013)
Follow up • Chronic leukemias • Recommended check ups every 6 months • Acute leukemias • Every month after treatment for the first year • To monitor for health changes and treat as necessary • Monitor for return of cancer or the worsening of chronic Leukemias • Physical exam, blood tests, bone marrow tests, other tests as indicated. (National Cancer Institute, 2013).
Counseling/ Education • Support groups for patient and family can be helpful with resources, education and support. Immunizations need to be up to date ie: flu, pneumovac • At time of diagnosis: How to care for yourself before treatment, avoidance of infection, rest, planning. • During therapy: Managing your symptoms, sexual changes and prevention of pregnancy, preventing and treating infections, preventing clotting, bleeding, staying active, relaxation, limiting visitors without isolation, coping with stressors. • After treatment: Keeping follow up appointments, normalizing life again, monitoring for infections, “late effects” • Stop smoking! (National Cancer Institute, 2013).
Consultation/ Referral • Hematologist • Medical Oncologist • Pediatric oncologist • Radiation oncologist • Oncology nurse • Social worker • Registered dietician • Gastroenterologist, Nephrologist, Neurologist as needed • Cancer Centers * * Cancer centers are recommended for Leukemias, especially acute forms • Gynecologist • Complementary therapists: Acupuncture, Reiki, Meditation, Hypnosis, Aromatherapist • Hospice • Pain management • Cancer rehabilitation • Home care • Psychiatrist, counselors • Physical therapy • Spiritual/ Religious counselors (National Cancer Institute, 2013).
Questions 1. True or false? The goal of acute Leukemia is remission. 2. True or false? The etiology of most types of leukemia is unknown. 3. What is the median age for AML and CLL? a.) 30 b.) 50 c.) 10 d.) 70 4. What is the most common type of leukemia in children? a.) ALL b.) AML c.) CML d.) CLL
Questions 5. A patient presents to the office with newly diagnosed Chronic lymphocytic leukemia. They want to know when their therapy will begin. You tell them: a.) Treatment begins right away b.) Early treatment is not recommended for those patients not at high risk c.) Treatment begins when the patient is infection free 6. What types of leukemia would a Bone marrow transplant be the only curative measure? a.) ALL and CLL b.) AML and CML c.) ALL and AML d.) CLL and CML 7. A patient comes into the office and is concerned about the staging of their leukemia. You tell them: a.) Blood cancers are already widespread, so there is no staging like tumor related cancers. b.) Their cancer is staged based on their age. c.) Their cancer is based on the amount of symptoms they are currently experiencing.
Questions 8. The difference between lymphoma and leukemia is: a.) Leukemia occurs in the white blood cells and lymphoma occurs in the marrow b.) Leukemia occurs in the white blood cells and lymphoma occurs in the lymph tissue c.) The two are exactly the same. 9. A 32 year old female who has been in remission for 5 years with ALL comes to the office because she has not been able to get pregnant. You tell her: a.) Keep trying, it will happen. b.) She should not ever have children due to the risk of relapse. c.) She may have infertility issues due to her treatments, and should see an OB/GYN right away. 10. A 42 year old who was recently diagnosed with AML. Which of the following would least likely be a risk factor for this type? a.) gender b.) smoking c.) chemical exposure d.) family history
References American Cancer Society. (2014). Leukemia – Acute Lymphocytic (Adults). Retrieved from http://www.cancer.org/acs/groups/cid/documents/webcontent/003109-pdf.pdf. Burns, C. (2013). Pediatric Primary Care (5th ed.). Philadelphia: Elsevier Health. Domino, F. (2014). The 5- Minute Clinical Consult (14th ed.). Philadelphia: Lippincott Williams & Wilkins. Dunphy, L. (2011). Primary Care: The art and science of Advanced practice nursing. (3rd ed.). Philadelphia: F.A. Davis Company. Katzung, B., Masters, S., & Trevor, A. (2012). Basic and Clinical Pharmacology (12th ed.). New York: McGraw Hill Medical. Larson, R. (2014). Leukemia. UpToDate. Retrieved from http://www.uptodateonline.com. Lee, S. (2009). Pathology 2: Leukemia chart. NCNM. Retrieved from http://ncnmnotes.blogspot.com/2009/12/pathology-ii-leukemia-chart.html. National Cancer Institute. (2013). Childhood Acute Lymphoblastic Leukemia Treatment. National Institute of Health. Retrieved from http://www.cancer.gov/cancertopics/pdq/treatment/childALL/Patient/page1.