Download
1 / 68
1.73k likes | 3.58k Views
Corneal laceration. Alireza Peyman, MD. Surgical repair. The primary goal is to achieve a watertight globe and maintain structural integrity . Secondary goals include: removing any disrupted lens fragments and vitreous repositioning any uveal tissue

E N D
Corneal laceration Alireza Peyman, MD
Surgical repair • The primary goal is to achieve a watertight globe and maintain structural integrity. • Secondary goals include: • removing any disrupted lens fragments and vitreous • repositioning any uvealtissue • relieving vitreous incarceration • removing any intraocular foreign bodies • restoring normal anatomic relationships
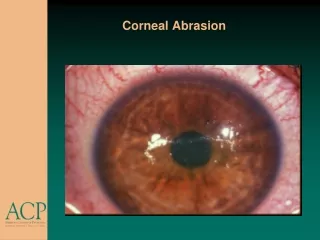
Partial-Thickness Corneal Lacerations • Must be examined carefully to rule out any rupture of Descemet • Seidel testing • Modified Seidel testing
If the wound edges are in good apposition with no wound gape, pressure patching with the use of prophylactic topical antibiotics is sufficient.
If the wound is unstable, a bandage soft contact lens may be used to support the wound
Partial thickness laceration with gape • Sutures may be used to re-approximate the wound margins. • In these settings, properly placed sutures will minimize scarring and perturbation of the ultimate surface corneal topography
BANDAGE SOFT CONTACT LENS • For small, self-sealing corneal perforations, a bandage contact lens may be sufficient • Such lacerations include nondisplaced, beveled, self-sealing wounds. • If aqueous leakage persists for more than 24 hours or there is progressive shallowing of the anterior chamber, more definitive treatment should be undertaken
In cases that respond satisfactorily, the contact lens should be kept in place until the wound has stabilized (usually 3–6 weeks). • A protective shield should be worn at all times. • Topical antibiotic prophylaxis and cycloplegia are recommended with the lens in place.
TISSUE ADHESIVE. • Tissue adhesive may be useful for puncture wounds with small amounts of central tissue loss and selected small lacerations. It is not routinely utilized.
SUTURE REPAIR OF SIMPLE CORNEAL LACERATIONS • The primary goal of corneal suturing is to achieve a watertight wound. • Secondary goals include • minimizing scarring • restoring normal anatomic relationships • reconstructing the normal corneal topographic contours
For a wound that is less stable, a viscoelastic may be irrigated into the anterior chamber either directly through the wound itself or through a separate limbal paracentesis incision
viscothrough the wound or through a paracentesis incision will help
To form the chamber: • Balanced salt solution or air may also be used to re-form the anterior chamber. • In most cases, a limbal paracentesis with a A 15-degree sharp microsurgical knife is preferred because it will minimize disruption of the wound edges and permit better access as the case proceeds
Temporary sutures • Temporary sutures may be used if the initial placement of deep definitive sutures would cause loss/flattening of the anterior chamber. • The number of temporary sutures should be minimized, however, to prevent undue trauma to the wound margins
Technique and material • For corneal suturing, 10-0 monofilament nylon on a fine spatula-design microsurgical needle is used. • The simplest method is to progressively halve the wound with simple interrupted sutures.
Corneal sutures should be • 90% to 95% depth through the stroma • 1.5 mm in length • of equal depth on each side • Shallow sutures create internal wound gape, whereas sutures of unequal length and depth on each side of the wound result in wound override.
Deep suture placement equidistant from the wound margins gives excellent wound approximation
Full-thickness sutures may create a conduit for microbial invasion
For shelved lacerations, sutures should be placed equidistant with respect to the internal aspect of the wound to achieve good wound apposition
When using a running suture for a nonlinear laceration, the suture should be placed with respect to a straight “regression” line
multiple interrupted sutures and tissue adhesive or patch graft
Iris incarceration • A peaked pupil signals tissue incarceration • Macerated, feathery, devitalized, or depigmented iris should be excised • The prolapsed tissue should be evaluated for any signs of surface epithelialization. • In this case, it should be excised to prevent any epithelial cells from proliferating in the anterior chamber
In general, tissue that has been prolapsed for longer than 24 hours should be excised to avoid infection; • however, if the tissue appears healthy, it may be replaced with caution.
Repositioning • Pharmacological • Midriatics • Myiotics • Mechanical • simply deepening • Viscoelastics through the paracentesisor the wound • a spatula or irrigating canula may be passed through the paracentesis site and used to directly sweep incarcerated tissue
Primary removal of the lens • Disrupted capsule and flocculent cortical material liberated into the anterior chamber. • In cases in which vitreous is involved with lens remnants, this may be best addressed in the initial surgery. • When it is clear that a lens is cataractous and surgical visualization is good, the lens may be removed in the primary operation.
For large lacerations with structural deformation, sutures should be placed to restore wound integrity before rigorous exploration of the globe • Initially, the limbus should be reapproximated with 8-0 or 9-0 nonabsorbable nylon or silk sutures.