Download
1 / 19
320 likes | 1.73k Views
Bell’s Palsy. Dr. Ali Tahir. Facial nerve. Sir Charles Bell (1774-1842) first studied the facial nerve anatomy A mixed nerve, with motor, sensory, special sensory & secretomotor fibers Motor muscles of facial expression Sensory concha and retro-auricular skin

E N D
Bell’s Palsy Dr. Ali Tahir
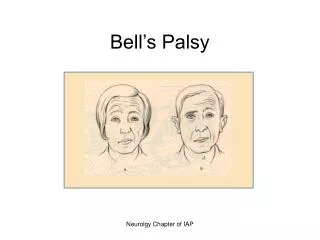
Facial nerve • Sir Charles Bell (1774-1842) first studied the facial nerve anatomy • A mixed nerve, with motor, sensory, special sensory & secretomotorfibers • Motor muscles of facial expression • Sensory concha and retro-auricular skin • Special Sensory taste sensation • Secretomotor lacrimal, sublingual, submandibular glands & some in nose & palate
Branches • Greater superficial petrosal nerve: • Nerve to stapedius: • Chorda tympani: • Communicating branch: • Posterior auricular nerve: • Muscular branches: • Peripheral branches: “Pesanserinus”
Bell’s palsy Bells palsy is an acute lower motor neuron paralysis of the face • Idiopathic • Diagnosis of exclusion • 10-30 per 100,000 • Usually young adults • Peripheral neuropathy
Pathophysiology • Exact cause unknown • Inflammation/oedema of facial nerve with demyelination, usually in stylomastoid canal • May be immunologically mediated & associated with infection, usually HSV • Other causative micro-organisms can be VZV, EBV, CMV, HHV-6, HIV, HTLV-1 or bacterial otitis media, lyme disease • Vascular ischemia
Predisposing factors • Pregnancy • Hypertension • Diabetes • Lymphoma • Hereditary
Clinical Features • Twitching, weakness, paralysis of face, dryness of eyes/mouth, disturbance of taste/hearing • Acute onset • Generally Unilateral • Acute onset < 48 hours • Paralysis of upper and lower face • Diminished blinking • Dryness, erosion, ulceration of cornea & potential loss of the eye
Clinical features • occasionally: • Pain in ear or jaw may precede the palsy • Facial numbness • If lesion is proximal to stylomastoid canal, there may be hyperacusis, loss of taste/lacrimation • Upto 10% have family history • Upto 10% have recurrent episodes
Diagnosis • Exclude other causes of facial palsy such as • Stroke • Trauma to facial nerve • Tumours affecting the facial nerve • Inflammatory disorder affecting the facial n. • Multiple sclerosis • Connective tissue disease • Sarcoidosis • MelkerssonRoenthal Syndrome
Examination • A full neurological examination to exclude a stroke or lesions involving other cranial nerves • Examination of facial nerve • Corneal reflex • Close eyes against resistance • Raise eyebrows • Raise lips to show teeth • Try to whistle
Examination • Ear & mouth examination to rule out Ramsay-Hunt Syndrome which causes lesions in the palate & ipsilateral ear & facia palsy • Ear examination for any discharge or middle ear infections
Investigations • Test for degree of nerve damage • Facial nerve stimulation • Needle electro-myography • Test for loss of hearing • Pure tone audiometry • Test for loss of taste • Test for balance • Schirmer’s test • CT/MRI to rule out any tumour • B.P • Blood complete
Investigations • Blood sugar • Tests for HSV, HIV or other viral infections • Serum ACE to rule out sarcoidosis • Serum ANA to exclude connective tissue disease • ELIZA to rule out lyme disease
Management • Observation • Upto 85% improve spontaneously within a few weeks • Medical treatment • Steroid such as prednisolone (80-90% recovery) • Anti-viral agents (aciclovir) • Facial rehabilitaion