Download
1 / 11
120 likes | 398 Views
HEMOPHILIA. MISHA MAZHAR 2k10-NUST-BS-V&I-54. OVERVIEW. An inherited bleeding disorder. Occurs in two forms. Hemophilia A. Hemophilia B. WHAT CAUSES HEMOPHILIA?. Mutations in F8 or F9 genes. Leads to lack of proteins made by these genes.

E N D
HEMOPHILIA MISHA MAZHAR 2k10-NUST-BS-V&I-54
OVERVIEW An inherited bleeding disorder Occurs in two forms Hemophilia A Hemophilia B
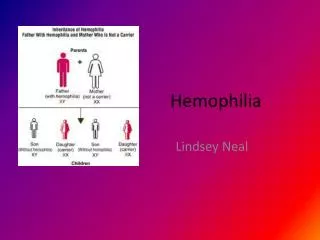
WHAT CAUSES HEMOPHILIA? • Mutations in F8 or F9 genes. • Leads to lack of proteins made by these genes. • F8 responsible for making the blood clotting factor VIII • F9 responsible for making the blood clotting factor IX
HEMOPHILIA A • Classic Hemophilia • X linked recessive hereditary disorder that is due to defective or deficient factor VIII HEMOPHILIA B • Also known as christmas disease • X linked recessive hereditary disorder that is due to the defective or deficient factor IX
DIAGNOSIS • Indications for Testing • Spontaneous or prolonged bleeding suggestive of coagulation disorder • Family history of hemophilia • Acute or recent onset bleeding accompanied by prolonged partial thromboplastin time (PTT)
Initial Laboratory Testing for Coagulation Disorders • CBC with platelet count – normal in hemophilia A, B • Prothrombin time (PT)/PTT • PT – normal in hemophilia A, B • PTT – prolonged in moderate and severe hemophilia • May not be prolonged in mild cases or in female carriers • Prolonged PTT that corrects in a mixing study suggests factor deficiency • PTT that does not correct with mixing study suggests an inhibitor • Incubated mixing studies are often necessary to identify FVIII inhibitors • Thrombin clotting time and plasma concentration of fibrinogen – normal in hemophilia A and B
CLINICAL MENIFESTATIONS • Frequency and severity of bleeding are related to F VIII levels
Hemarthrosis • Bleeding into the joints • The bleeding causes distension of the joint spaces, significant pain, and over time, can be disfiguring. • Clinically: • Aura: tingling warm sensation • Excruciating pain • Generally affects one joint at the time • The knees and ankles are most often affected • If treated early it can subside in 6 to 8 hrs and disappear in 12 to 24 hrs.
CLINICAL MENIFESTATIONS • Bleeding into the muscles may occur with hematoma formation. • Bleeding from the mouth or nosebleedsmay occur. Bleeding after dental procedures is common, and oozing of blood from the gums may occur in young children when new teeth are erupting. • Bleeding from the gastrointestinal tract can lead to blood in stool. • Bleeding from the urinary tract can lead to blood in the urine (hematuria). • Intercranial hemorrhage (bleeding into the brain or skull) can lead to symptoms such as nausea, vomiting, and/or lethargy. • Increased bleeding after surgery or trauma is characteristic of hemophilia.
MEDICATIONS • Slow injection of hormone desmopressin (DDAVP) into a vein to stimulate a release of more clotting factor to stop bleeding. • Antifibrinolytics such as Aminocaproic acid (Amicar) and tranexamic acid (Cyklokapron) assist your clotting by slowing down the ongoing destruction of clots. These medications are useful in oral bleeding in either hemophilia A or B. • An IV infusion of factors may also be givenpurified Factor VII or IX depending on the type of hemophilia.