Download

1 / 20
200 likes | 332 Views
PUBLIC HEALTH NETWORK MEETING. WELCOME. RASH DECISIONS. Agenda. 12.30-12.40 Welcome & introduction 12.40-1.15 Measles Outbreaks – recent experiences from Cornwall & Bath Mark Kealy & Mary-Ann McKibben & Jo Williams 1.15-1.25 Questions 1.25-1.50 Meningitis study Toyin Ejidokun

E N D
PUBLIC HEALTH NETWORK MEETING WELCOME RASH DECISIONS
Agenda • 12.30-12.40 Welcome & introduction • 12.40-1.15 Measles Outbreaks – recent experiences from Cornwall & Bath • Mark Kealy & Mary-Ann McKibben & Jo Williams • 1.15-1.25 Questions • 1.25-1.50 Meningitis study • Toyin Ejidokun • 1.50-2.00 Questions
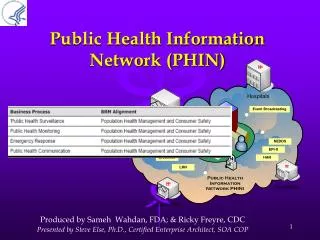
Evaluation of an early diagnosis model for meningitis Dr Toyin Ejidokun1, Mrs Cate Johnson2, Mrs Grace Magani2, Ms Cate Conlon3, Mrs Faustina Montsho-Hammond3, Ms Julie Mann3, Mrs Wendy Ainsworth4, Mrs Sarah King4 1Consultant in Communicable Disease Control, Avon, Gloucestershire & Wiltshire Health Protection unit 2Health Protection nurse, Gloucestershire Health protection team 3Health Protection nurse, Avon Health Protection team 4Health Protection nurse, Wiltshire Health Protection team
Notifications of meningococcal diseaseEngland and Wales 1912-2004
Introduction • Bacterial meningitis remains an important cause of serious morbidity and mortality in children and young adults despite the significant success of the national immunisation strategy against meningococcal C disease • The ability to make a prompt and accurate diagnosis of acute bacterial meningitis is important for starting effective treatment and implementing public health protection measures • Gold standard tests such as cerebrospinal fluid (CSF) examination may not be done because of contraindications • Test results also depend on the stage of the illness when the sample was taken and may not be very helpful • These factors demonstrate the importance of considering other parameters in addition to, or in place of CSF findings to assist in making an early diagnosis
Why is meningococcal disease important? • Substantial burden of disease • Dramatic onset, rapid progression • Difficult diagnosis for public and professionals • High public profile • Causes outbreaks • Treatable, preventable – potential health gain
Clinical presentation • Meningitis • case fatality 5% • fever, vomiting, drowsiness, headache, photophobia, neck stiffness • myalgia, joint pains, rash • Septicaemia • case fatality 20% • rash and shock • Most cases have mixed presentation
Symptoms of meningococcal disease Meningitis Research Foundation www.meningitis.org.uk
Serogroup B and C cases 1998 – 2005England and Wales Men C campaign
Method • To test how useful a scoring system • which uses symptoms, clinical signs, laboratory tests results and epidemiological information • is in making an early diagnosis of meningitis
Data collection • General demography: age, gender • Level of consciousness, presence & type of rash • Blood results: White cell count, glucose, C-reactive protein, blood culture, Antigen tests, Polymerase Chain Reaction • CSF results: protein, white cell count, glucose, protein, culture, antigen tests, Polymerase Chain Reaction • Throat swab culture • Urine antigen test, stool culture • Antibiotics before admission • Meningococcal C vaccine • Epidemiology data: Links to previous cases & type of link, student?, year of study, institution type, type of residence, outcome of illness episode, postcode of residence, PCT, Local authority
The study process…….. • Health Protection Unit staff to collect information on all suspected probable bacterial and viral meningitis cases • Where: 3 regions: London, West Midlands and the South west • Duration: 12 month period • Number of cases: at least 207 • Data analysis: Excel and Stata • Data validation: by Regional Epidemiological unit and compared to other sources e.g. Lab Base, CoSurv, official notifications and Hospital Episode Statistics
Some definitions……….. • Probable case: where the most likely clinical diagnosis is meningitis • Confirmed case: where bacteria, bacterial antigen and/or DNA is identified in cerebrospinal fluid (CSF); bacteria or viruses obtained from culture of CSF and or clinical and/or laboratory diagnosis of meningitis accompanied by microbiological evidence of pathogen from another site e.g. blood, throat swab, skin or faeces
So far we have identified…… • Health Protection Team study leads: very important links with local clinicians and public health on-call staff • Health Protection Unit study leads • Regional lead study scientist • Regional epidemiologist leads • Overall lead study scientist: Becky Close
Progress to date • Pilot data collection started in March 08 • Database for collation of data agreed between lead study scientist and regional lead study scientist • Process for sending data to lead study scientist agreed • Awaiting trust ethical approval from participating trusts • Aim to start proper study data collection on 1 July 2008
Thank you for your attention • Any questions?