Download
1 / 64
640 likes | 657 Views
Explore the various factors influencing speech sound acquisition, including genetic factors, environmental influences, familial and personal factors, language skills, tongue thrust, sensory variables, and anatomical, neurological, and physiological factors.

E N D
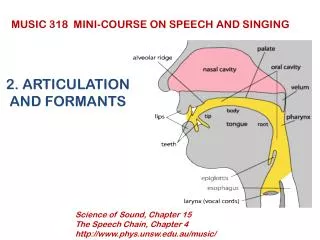
VARIABLES RELATED TO • ARTICULATION AND PHONOLOGICAL DEVELOPMENT AND PERFORMANCE
I. INTRODUCTION** • There are a number of variables associated with speech sound acquisition. • Research: can only demonstrate correlation, not cause-and-effect-relationships.
Some genes may affect both** language and speech • Language and speech disorders may occur alone or together • “He sounds just like I did when I was a kid”
Reading disabiity SSD Language Impairment Genetics
Decreased phonological awareness skills** • Have been implicated in poor reading ability in young children
**Goldstein, H., et al. Efficacy of a supplemental phonemic awareness curriculum to instruct preschoolers with delays in literacy development. Journal of Speech-Language-Hearing Research, 60, 89-203.
Hayiou-Thomas et al. When** does speech sound disorder matter for literacy? The role of disordered speech errors, co-occurring language impairment and family risk of dyslexia. Journal of Child Psychology and Psychiatry, 58:2, 197-205.
Baron et al., 2018 (August). Children with dyslexia benefit from orthographic facilitation during spoken word learning. Journal of Speech, Language, and Hearing Research, 61, 2002-2014.
III. ENVIRONMENT** • Role models are a variable • Health is a factor too—is there health insurance? • Preschool opportunities?
Socioeconomic status…** • Has a significant effect on the development of phonological awareness skills • Children from mid- and high-SES backgrounds outperform children from low-SES backgrounds
IV.FAMILIAL AND PERSONAL FACTORS** • Birth order & # of siblings—research inconclusive • Gender—SSDs more common in boys • Age—between 4-6 yrs. old, most children begin to sound like adults; improvements can be made till 8yrs.
Youtube video** • People with Down Syndrome speak out • AJ+ • What errors do you hear? Write them down as you listen.
V. LANGUAGE SKILLS** • Many children have problems with BOTH language and speech—there is a synergistic relationship • Children with SSDs may use incomplete sentences, shorter utterances, and less complex language • As sentence length and complexity ↑, speech sound errors ↑
Speech sound errors especially increase when children are trying to produce:
V. TONGUE THRUST** • A. Introduction • Also called reverse swallow • Certain manner of swallowing and tongue placement in oral cavity during rest
Habitual or obligatory** • obligatory=organic/physical—e.g., enlarged tonsils or adenoids that partially block the posterior airway passage • Orofacial myology (tx for TT)
Orofacial Myology is:** • Study of relationships among dentition, speech, and nonspeech tongue and facial muscles
B. Characteristics of Tongue Thrust** • During swallowing, tongue comes forward--tip in contact with lower lip • At rest, tongue is carried forward—tip is between or against anterior teeth while mandible is open
Youtube video** • Tongue thrust: Children’s crooked teeth • Dan Hanson • It’s a little mean but really shows tongue thrust
ASHA’s Position:** • TT co-occurs with speech problems in some clients • Assessment and treatment of TT is within SLP’s scope of practice • SLP must be highly trained and work on a team with appropriate professionals such as dentists, orthodontists, and allergists
VI. SENSORY VARIABLES** • A. Oral Sensation • Looked at oral stereognosis or form recognition • B. Hearing Loss
C. Auditory Discrimination** • Previously, believed that AD had to precede correct production of a sound • Research: training discrim only affected discrim, but training correct production helped both AD and production! • Get into production!
VII. ANATOMIC, NEUROLOGIC, AND PHYSIOLOGIC FACTORS** • A. Anatomic Structures • 1. Soft palate —may have VPI. Mobility and enough tissue are very important • Need good VP closure for pressure consonants especially—fricatives, affricates, stops • May use glottal stops for other sounds • May also have nasal emission and hypernasality
2. Nasopharynx** • Adenoids/nasopharyngeal tonsils • May be hypertrophied; child is possibly hyponasal • Can compensate for short or partially immobile soft palate by assisting with VP closure • Can block Eustachian tube opening into nasopharynx, depriving middle ear of ventilation
3. Hard palate; cleft, cancer have** impact • 4. Teeth —extra or supernumerary teeth (or Class I, Class II, Class III malocclusion; pp. 99-100; please know for Test 2) • 5. Lips (cleft can affect speech) • 6. Tongue