Download
1 / 31
310 likes | 441 Views
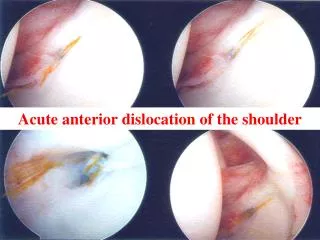
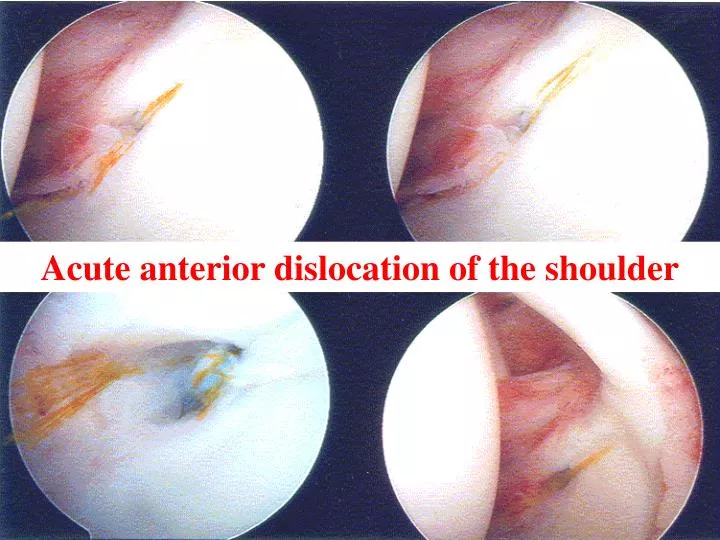
Acute anterior dislocation of the shoulder. Anatomy Stability: - ball & socket = compression in concavity effect Bone - big head – small cup = unstable Menisci - labium = ↑ depth of cup by 20% Ligaments - glenohumeral & capsule

E N D
Anatomy Stability: - ball & socket = compression in concavity effect Bone - big head – small cup = unstable Menisci - labium = ↑ depth of cup by 20% Ligaments - glenohumeral & capsule Muscles - rotator cuff & biceps = holds ball in cup Primary Movers - Deltoid, Pec. major & Lat. Dorsy = subluxing forces Dynamic - proprioceptive feedback
Pathophysiology (Lazarus 1996) Chondro-labral defect causes a 65% reduction in stability in the direction of the defect Deficiency of the ant. inf. capsulolabral complex Fracture of ant. lip of glenoid = 15% Detachment of labarum/capsule = 15% Tear of glenohumeral ligaments = 54% Avulsion of subscapularis and ligs of humerus (HAGL) To prevent the persistence of the defect it needs to be repaired Arthroscopically Open
Acute Injury Something breaks or tears and therefore can be repaired. Repair is better than reconstruct Repair is easier than reconstruct Chronic Instability has additional plastic deformation of the capsule and glenohumeral ligaments therefore needs to be shortened Restoring the normal functional anatomy is impossible
Conservative Treatment Rowe – JBJS, 1957 324 young patient with ant. dislocations • 94% had recurrence if < 20 years old • 62% had recurrence if < 30 years old • 14% had recurrence if > 40 years old Burkhead & Rockwood (text book) 40 patients with acute dislocation & vigorous rehabilitation • Only 16% had good or excellent result (1 in 6) Deny & Drew – Injury, November 2002 • 21% of all patients presenting with shoulder dislocation had previous dislocation in 1 year • 43% in patients 15-22 years had re-dislocations
Non operative treatment of shoulder dislocation in young athletes Arciera – J Arthroscopy, 1995 De Beardino – J South Orthopaedic Ass, 1996 Haelen – J Arch Orthopaedic Trauma Surgery, 1990 Hovelius – J Orthopaedic Science, 1999 Wheeler – J Arthroscopy, 1998 Kirkby – J Arthroscopy, 1999 all over 80% recurrence rate Non operative treatment is unacceptable
Prospective Randomised Study Bottani etc.–Military Personnel Medicine Vol 30 No 4 2000 First Time Acute Traumatic Shoulder Dislocation Stabilisation V’s Non Operative: Follow up in 36 months 24 patients aged 18-26y. 14 Non Operative – rehab immobilised 4 weeks 9 of 12 non operative had instability (75%) (6 open Bankart repair) 10 ASC Bankart repair with bioabsorbable tack <10 days 1 of 9 operated patients had instability (11%)
Comparison of Arthroscopic & Open Stabilisation Sample Size Follow Up Recurrence ASC Open ASC Open ASC Open Steinbeck 1998 30 32 36 40 17 5 Field 1999 50 50 33 30 8 0 Cole 1999 37 22 52 55 16 9 Hayes etc 1999 44 13 29 29 12 4 Conclusion Arthroscopic repair for chronic instability is inferior to open repair ? Due to plastic deformation Chronic anterior instability
Arthroscopic Techniques for Primary Dislocations 1982 Johusa – with staples 1987 Morgen & Badenstab – transglenoid sutures 1991 Caspari -Cannulated bio-absorbable tacks 1993 Wolf & Snyder – suture anchors = difficult 1989 Wheller - ASC staple 1993 Gohlke - Suture anchors 1994 Arciera - ASC transglenoid 1996 Speer - Bio-absorbable tack 1999 Wintzell - ASC lavage 2000 Introduction of a multitude of new gadgets & anchors
Arthroscopic Repairs Einoder, 1984 Knee Club • Described Arthroscopic transglenoid sutures using: • K wire with eye (ACL) introduced via anterior portal • Sucking tube • Sutures tied over infraspinatus fascia or spine of scapula Results • 4 out 5 patients returned to the same level of sport with no re-dislocations
Boszotta & Helperstorfer – Arthroscopy, July 2000 Transglenoid suture repair for initial Ant. dislocation 72 patients (1988-95) 61♂ 11 ♀ Aged 19-39 34% = Bankart lesion (6 with bone) 66% = Avulsion of capsulolabral complex Results 7% = Redislocation all due to trauma (severe in 2 out of 5) 85% = Returned to unrestricted pre injury sporting activities
Randomised Studies Asc. Stabilisation V’s Non Operative Arciera et. al. – A.J. Sports Med., 1994 • 32 military men with acute 1st up dislocation, Average of 32 months follow up 15 patients – non operative – 80% redislocated 21 patients – transglenoid suture – 14% redislocated Bottony & Wilkings etc. A.J. Sports Medicine 2000 • Patients with acute traumatic first time shoulder dislocation 14 young patients – non op, 75% redislocation 10 young patients – Asc. Bankart repair, 10% redislocation
Asc. stabilisation Dara & Gerber – Journal of Shoulder & Elbow, 2000 20 shoulders Av 3 year follow up Recurrences occurred in patients who were chronic dislocators i.e. <30% Therefore now do open surgery for recurrent dislocations Asc. surgery for acute dislocations De Beardino et al – An J. Sports Med., 2000 49 1st up acute post traumatic Shoulders dislocation Average 37 months follow up Tack anchor. 6 Patients re-dislocated (13%) +4 had open surgery
Bozzotta & Helpastorger (Austria) – J. Arthroscopy, 2000 Arthroscopic Transglenoid Suture Repair for Initial Ant. Shoulder Dislocation • 72 Patients 61♂ 11♀ - Sporting ambitious patients 25 Patients Bankart lesion (6 with bone) 43 Patients Capsulolabral avulsion Results • 5 patients Re dislocated 2 had significant trauma 3 had insignificant trauma = 4% • Therefore results of primary repair are better than surgery for recurrent dislocation • But transgleniod repairs are obsolete
Against …Arthroscopic Repair Roberts, Taylor, Brown, Hayes, Saies (Adelaide) Journal of Shoulder & Elbow, September 1999 56 acute 1st up shoulder dislocations 2½ year post operative and return to Australian Rules Football Operations: Asc. suture repair – 70% recurrence Asc. Bankart repair with tack – 38% recurrence,.. Open repair & copsular shift – 30% recurrence Therefore Asc. treatment alone not good enough
Cole & Warner – Clinical Sports Medicine 2000 Arthroscopic V’s Open Bankart Repair For Traumatic Anterior Shoulder Instability % Asc. treatment modalities are increasing due to: Better understanding of the pathophysiology Better pre operative evaluation of the injury (i.e. patient selection) New surgical techniques Better instrumentation Better anchors
Protocol for Acute Repair Mature & active person 15 to 50 years old First episode of glenohumeral dislocation Reduced on field, first aid, club Dr or DEM Examination & X-ray Informed consent – time off work - outcome Examination under GA ASC of glenohumeral joint, check rotator cuff as well Acute repair of all demonstrable tears or fractures restore normal anatomy Rehab activity – collar & cuff, physiotherapy Avoid ext. rotation and abduction for 6 weeks Return to contact sport in 12 weeks
Investigations • Plain x-rays • CT scans if complicated associated feature • MRI rarely – get more information from Asc. • Examination Under GA Supine load shift test with arm at 80° abducted compared with normal shoulder 1+ ball to rim 2+ ball riding over rim with spontaneous reduction 3+ ball stays dislocated • Arthroscopy
Arthroscopic Repair Procedure Patient Position General Anaesthetic Beach Chair with arm held by assistant Lateral position with arm in traction & shoulder abducted Shoulder examined, degree & direction of instability noted Portals = 2 or 3 • Posterior portal • Ant. sup portal • Ant inf portal (occasionally) • Injury assessed & debrided • Repair method selected
Rehabilitation • Minimal in first 4 weeks No ext rotation Abduction less than 45° Pendulum exercises Isometric resistance exercises • Graduated in 4 – 8 weeks ↑ ROM Graduated weight training • Return to sport Non contact = 6 weeks contact = 12 weeks
Arthroscopic V’s Open Bankart Repair Advantages Accurate diagnosis of all structures Less morbidity/pain Small scars Faster recovery Sooner return to activities Less restriction of movement Disadvantages Need all the equipment Technically demanding Long learning curve Lack of versatility Higher failure rate arthroscopic = up to 33% - open = less than 10%
Stern Jozrawi Rastolazzi – Arthroscopy Oct. 2002 Advantages V’s Disadvantages of Asc. Repair Advantages ↑ cosmesis ↓ morbidity ↓ stiffness Easy revision Disadvantages 1) Reluctance to refer patient immediately 2) Difficult operation 3) Expensive instrumentation 4) Biological healing time is not accelerated 5) Same post operative restrictions
Problems • Difficulty convincing Club Trainers, Physicians, sporting club Doctors & DEM staff to refer the young athlete within 2-3 days. • Time consuming discussions convincing patient to have the operation rather than early return to sport. No problem advising a recurrent dislocators to have a stabilisation procedure at the end of a sporting season. • Mostly after hours surgery with staff who are not familiar with the operation and instrumentation.
Arthroscopy of Shoulder 1935 – Japanese Surgeons arthroscoped, shoulders 1960s – Curiosity activity in the western world 1970s – Diagnostic Asc. examination è open surgery 1980s – Simple Asc. techniques èfor simple problems 1990s – ↑ Instrumentation & tacks è more tried it. 2000s – ↑ Techniques & anchors – Can be done by any surgeon skilled in arthroscopic techniques
Shoulder reduced on field, first aid room or DEM then referred Treatment History 1970s - Conservative for all 1st up unless fractures with Bristows or Bankart repair for recurrences 1980s - Asc. transglenoid sutures tied over spine of scapula or muscle fascia 1990s - patient in lateral position with arm in traction or patient in Beach chair position multiple, tacks and sutures surtac screw tack anchors etc. 2000 - better anchors and sutures have made the procedure available for all surgeons experienced in arthroscopic technique
Conclusion Asc. repair of the Capsulo-ligamentous injury to the shoulder is a simple procedure for a surgeon skilled in arthroscopic technique Chronic instabilities have associated plastic deformity of the tissues that need to be addressed and this makes the result of a simple procedure unpredictable. An active young person with a first traumatic dislocation of the shoulder should have the damage repaired arthroscopically within 10 days of the injury