Download
1 / 42
450 likes | 696 Views
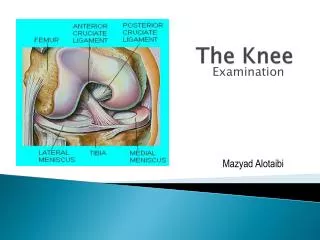
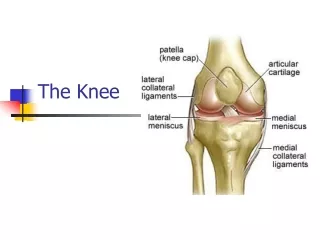
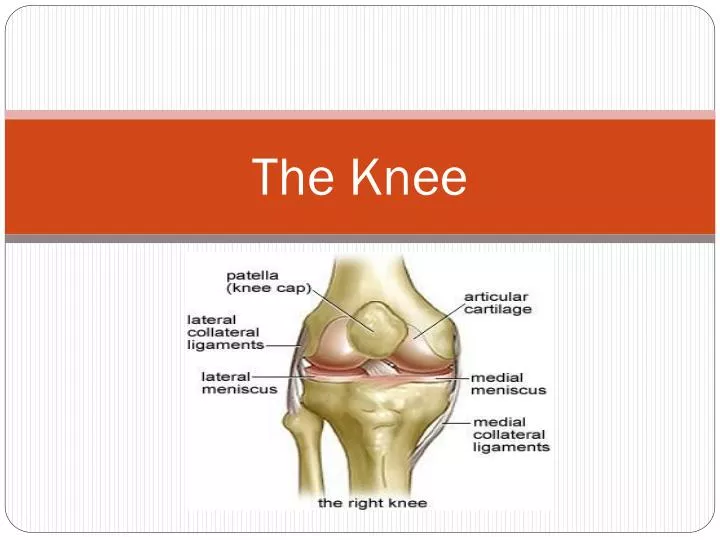
The Knee. Bony Anatomy . The knee is composed of four major bones The Femur Bone of the upper leg/thigh Condyles Tibia Medial bone in the lower leg Tibial plateau Fibula Lateral Bone in the lower leg Patella “Also known as kneecap” Sesamoid bone enveloped in the quadriceps tendon.

E N D
Bony Anatomy • The knee is composed of four major bones • The Femur • Bone of the upper leg/thigh • Condyles • Tibia • Medial bone in the lower leg • Tibial plateau • Fibula • Lateral Bone in the lower leg • Patella • “Also known as kneecap” • Sesamoid bone enveloped in the quadriceps tendon
Joints of the Knee • Tibiofemoral Joint • Weight-bearing, hinge joint • Held together with joint capsule and several ligaments • Patellofemoral Joint • Helps extend the knee
Cartilage • Two types of cartilage are found in the knee • Both are bathed in synovial fluid • Produced by the synovial membrane of the knee • Articular cartilage • Covers the ends of the tibia and femur • Covers the retropatellar surface • Meniscus • Wedge shaped cartilage • Aid in shock absorption, distributing forces and improving stability of the joint
Cartilage ~ Meniscus • Medial Meniscus • Between the medial femoral condyle and medial tibial plateau • “C” - shaped • Lateral Meniscus • Between the lateral femoral condyle and lateral tibial plateau • “U”- shaped
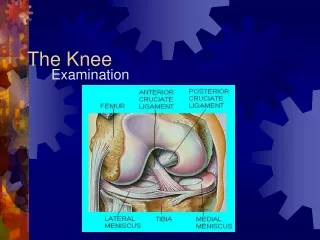
Ligaments of the Knee • Four major ligaments connect the tibia and femur • Two are located outside of the joint capsule • Medial Collateral Ligament (MCL) • Lateral Collateral Ligament (LCL) • Two are located on the inside of the joint • Anterior Cruciate Ligament (ACL) • Posterior Cruciate Ligament (PCL)
Ligaments ~ Collateral • Lateral Collateral Ligament (LCL) • Attaches the femur and the head of the fibula • Provides lateral stability • Only palpable ligament in the knee • Medial Collateral Ligament (MCL) • Attaches the femur to the tibia • Provides medial stability
Ligaments ~ Cruciate • Anterior Cruciate Ligament • Attaches the to the femur and anterior aspect of the tibial plateau • Prevents anterior translation of the tibia on the femur • Posterior Cruciate Ligament • Attaches to the femur and posterior aspect of the tibial plateau • Prevents posterior translation of the tibia on the femur • Cruciate is derived from Latin word meaning “cross” • ACL running Anterior-to-Posterior-Externally • PCL running Posterior-to-Anterior-Internally • Also help control rotation of the knee and medial/lateral stability
Muscular anatomy • Muscles that move the legs are the strongest in the body • Quadriceps • Extend the knee • Hamstrings • Flex the knee joint • Hip Flexors • Assist with knee flexion
Muscular Anatomy ~ Quadriceps • 4 muscles together join at the distal anterior thigh and attach the patella through the quadriceps tendon • Vatus Lateralis • Vastus Medialis • Vastus Intermedius • Rectus Femoris
Muscular Anatomy ~ Hamstrings • 3 muscles on the posterior aspect of the thigh are divided into two groups • Medial hamstrings • Semitendonosis • Semimembranosis • Lateral hamstring • Biceps Femoris
Muscular Anatomy ~ Hip Flexors • Two additional, long strap-like muscles in the thigh that assist with knee flexion • Sartorius • Gracillis • They attach to the anteriomedial tibia near the attachment of the semitendinosus • Area known as the pes ansurine
Knee Injuries • A wide variety of injuries can occur to the knee. Some of the most common are • Patellarfemoral • Patellar tendonitis • Sprains (MCL/LCL) • Ligament Tears (ACL/PCL) • Meniscus Tears • Epiphyseal injuries • Oshgood-Schlatter • Iliotibial Band syndrome • Fractures/dislocations of the patellarfemoral joint
Patellofemoral problems • Patellofemoral problems can be very challenging to the ATC and athlete • Usually caused by irregular tracking of the patella • It is not easy to identify the source of the problem • Classic complaints • Anterior pain/aching • Crepitus • Mild, or no swelling • Patella may appear to face inward, instead of forward
Patellofemoral Problems ~Recognition and Treatment • Recognition • Patellofemoral provocation test will help reproduce the symptoms for the athlete • Forward lunge • Step-down test • Treatment • Correct the suspected cause • Shoe inserts • Low-dye taping • Strengthening exercises • Specialized braces/taping
Patellar Tendonitis • Inflammation of the patellar tendon • Primarily seen in sports that involve jumping • Also called “jumper’s knee” • Symptoms • Anterior knee pain • inferior to the patella over the patella tendon • Minimal swelling may occur • Treatment • Activity modification • Non-impact activities • cycling, swimming • Stretching for tight quads • Ice after activity • Bracing
Fat Pad Syndrome • Involves a region of fatty tissue lying deep to the patellar tendon • Hoffa’s fat pad • When inflammed can become confused with patellar tendonitis • Symptoms • Pain inferior to the patella • Movement aggravates the symptoms • Point tenderness and swelling anteriorly • Treatment • Strengthening exercises • Full extension is contraindicated • Specialized taping • Anti-inflammatory medicines
Collateral Ligament Sprains • Results of stretching and a valgus force to the medial tibiofemoral joint or varus force to the lateral tibiofemoral joint • Severity of the sprain is determined by grading scale Grade I – Grade III • Signs/Symptoms • Grade I • Mild tenderness over ligament • Usually no swelling • Pain when ligament is stressed at 30 degrees, but no ligamentous laxity • Grade II • Significant tenderness over the ligament • Some swelling • Pain and some ligamentouslaxitiy when stressed, but definite end point • Grade III • Complete tear of the ligament • Pain can vary • When the ligament is stressed, there is significant ligamentous laxity • Knee feels wobbly or unstable
MCL/LCL Sprains • Treatment of acute injuries with PRICE • After acute phase, rehab should begin • Special Test • Valgus/Varus stress test
ACL Tears • An ACL tear is when the ligament is completely torn and is no longer intact • ACL tears are more common among female athletes than make athletes • 1 of 10 college athletes, 1 of 100 high school athletes • Usually due to women using the quads more than men • Some athletic shoes can increase the risk of injury • There seems to be no connection of ACL size to injury
ACL Tears ~ MOI • ACL tears can be from contact or non-contact causes • Contact • Contact that causes a blow to the lateral knee or valgus force • Non-contact • Situations where the knee is loaded and combined with flexion, valgus force and rotation of the tibia on the femur can rupture the ACL in a non-contact manner
ACL Tears ~ Signs & Symptoms • Symptoms include the following • Hearing a “pop” • Rapid effusion • Nasuea • Pain • Many times if the ligament is tested within 5 minutes of injury, the examiner can get a better result • Lachman’s maneuver and Anterior Drawer test the integrity of the ligament • Positive signs usually indicate rupture • Diagnosis and MRI by orthopedic will confirm the injury
ACL Tears ~ Treatment • Acute Treatment • PRICE • Use an immobilizer that prevents movement of the joint • Athlete should be non-weight bearing • Referral to orthopedic physician for diagnosis • Surgical Reconstruction • Allograft vs. Autograft replacement • Rehabilitation from ACL reconstruction is typically 6+ months
PCL Tears • Occur when athlete’s fall on the flexed knee with the foot in plantarflexion • The tibia hits the ground first and is pushed back • Occurs less often than ACL tears • Signs & Symptoms • A positive sag test is a good indication that the PCL has been torn
PCL tear ~ treatment • Immediate care is PRICE • Referral to a physician if suspected • Surgery can be avoided in most cases • A strong rehab program and physical therapy are important • Specific quadriceps strength and endurance training can compensate for the torn PCL
Meniscus Tears • Can be torn when the knee is suddenly twisted and one or both menisci become trapped between the femur and tibia
Meniscus Tears ~ S & S/Treatment • Signs and Symptoms • Gradual swelling • Pain • Popping • Locking • Giving away • Treatment • Immediate care is ice and compressive wrap • Use of crutches may be necessary • Referral to physician if suspected for MRI • Surgery is not always required
Meniscus Tears ~ Treatment/Special Test • Non-surgical management • Physical Therapy • Increase muscles strength • Increases range of motion • Modified activity • NSAISDs • Time • Special Tests • McMurrays
Epiphyseal growth-plate injuries • Normally seen in skeletally immature athletes • Forces that would normally cause ligamentous injuries in adults could potentially damage the growth-plate injury in children and younger athletes. • These injuries can be quite serious so athletes may only return to play upon approval of the physician.
Osgood-Schlatter • This condition is a group of symptoms involving the tibial tubercle epiphysis • A small bump of the anterior tibia where the patella tendon attaches • The tibial tubercle is a growth center • Affects males 12-16 and females 10-14 • Usually caused by a inflammation of the layers of the tubercle • Fibrocartilage lines the layer underneath the tibial tubercle • Layers are loosely held together during the active growth years
Osgood-Schlatter • Signs & Symptoms • Pain • Swelling • Weakness in the Quads • Increased pain/swelling with activity • A visible lump • Sensitive to palpation
Osgood-Schlatter ~ Treatment • Management of this condition can be managed as long as the pain, swelling and flexibility are managed. • Additional treatment include • Prevention of progression • Knee pad • Neoprene sleeve • Icing after activity • Anti-inflammatory medicines • Stretching the hamstrings • Should pain continue or increase, refer to physician
Iliotibial Band Syndrome • IT Band syndrome involves inflammation of the thick band of fibrous tissue that runs down the side of the tibia, just below the knee • Bursa between the mucles/bones and IT band becomes inflamed and makes movement painful • Usually affects people who suddenly increase level of activity • Ex. Runners increasing mileage • Others who are prone are • People who overpronate • Have leg-length discrepancies • Are bowlegged
IT Band Syndrome ~ Treatment • Analyze athlete's gait and training program • Rule out mechanical problems • Proper footwear • Icing the painful area • Stretching • Reduce or modify activities until symptoms subside
Fractures • Usually a result of high-energy trauma • Patella fractures • Can occur from direct impact to anterior knee • Distal femoral or proximal tibia • Can occur with violent twisting or falls from heights