Download
1 / 17
170 likes | 288 Views
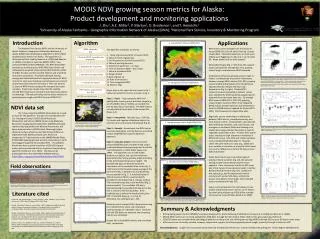
ANRS 1295/12160 - CIPRA KH001/10425 trial. The CAMELIA trial CAM bodian E arly vs. L ate I ntroduction of A ntiretrovirals. F.X. Blanc , T. Sok, D. Laureillard, L. Borand, C. Rekacewicz, E. Nerrienet, Y.Madec, O. Marcy, S. Chan, N. Prak, C. Kim, K.K. Lak, C. Hak, B. Dim,

E N D
ANRS 1295/12160 - CIPRA KH001/10425 trial The CAMELIA trialCAMbodianEarly vs. Late Introduction of Antiretrovirals F.X. Blanc, T. Sok, D. Laureillard, L. Borand, C. Rekacewicz, E. Nerrienet, Y.Madec, O. Marcy, S. Chan, N. Prak, C. Kim, K.K. Lak, C. Hak, B. Dim, C.I. Sin, S. Sun, B. Guillard, B. Sar, S. Vong, M. Fernandez, L. Fox, J.F. Delfraissy, A.E. Goldfeld. 22nd July 2010 LateBreaker Session B-1, XVIII IAS Conference, Vienna, Austria
HAART in TB-HIV: Early or late? Adapted from J Acquir Immune Defic Syndr 2007; 46: S9-S18.
WHO recommendations 2003: CD4 < 200/mm3: - Start TB treatment. - Start ART as soon as TB treatmentistolerated (between 2 weeks and 2 months) - Efavirenz-containingregimens 2010: - Start ART in all HIV-infectedindividualswith active TB, irrespectiveof the CD4 cell count. Strongrecommendation, lowquality of evidence. - Start TB treatment first, followed by ART as soon as possible afterwards (and within the first eightweeks). Strongrecommendation, moderatequality of evidence. - Use efavirenz as the preferred NNRTI in patients starting ART while on TB treatment. Strongrecommendation, highquality of evidence.
CAMELIA study design (2003-2004) • Prospective, randomized, open-label, two-armed trial with no placebo • Designed as a superiority trialto answer the question of the best timing for the introduction of HAART in severely immunosuppressed (CD4 ≤ 200/mm3) HIV-infected adult patients with newly diagnosed TB in Cambodia • 2 arms: late introduction of ART (reference arm: 8 weeks) vs.early(2 weeks) introduction of the same HAART • Primaryendpoint: survivalat the end of the trial (intent-to-treatanalysis) ANRS 1295/12160 - CIPRA KH001/10425 study
CAMELIA strategy Switch D4T to AZT ANRS 1295/12160 - CIPRA KH001/10425 study
CAMELIA key points • - 2 sponsors: French ANRS and U.S. NIH/DAIDS (CIPRA) • Partnership with Cambodian Health Committee • 5 study sites (rural and urban) in Cambodia • 661 patients were AFB+ at inclusion (pulmonary or extra-pulmonary TB) with CD4 ≤ 200/mm3 • 1st patient enrolled on January 31st 2006 • 6 DSMB meetings • Last patient enrolled on May 27th 2009 • End of the study: May 2010 ANRS 1295/12160 - CIPRA KH001/10425 study
CAMELIA recruitment 778 patients screened 117 patients not enrolled due to: - CD4>200 (n=78) - LFT impairment (n=24) - pregnancy (n=3) - TB treatment >1month (n=2) - CD4 >200 & LFT impairment (n=2) - death before randomization (n=2) - pregnancy & LFT impairment (n=1) - no CD4 at enrolment (n=1) - high bilirubine (n=1) - delay in blood sampling (n=1) - CD4>200 & pregnancy (n=1) - ART history & LFT impairment (n=1) 661 patients randomized 332 randomized to the EARLY arm 329 randomized to the LATE arm 282 culture + M.tb 38 culture - 12 NTM 294 culture + M.tb 31 culture - 4 NTM M.Tb: Mycobacterium tuberculosis; NTM: nontuberculous mycobacteria ANRS 1295/12160 - CIPRA KH001/10425 study
Patient characteristics at enrollment ANRS 1295/12160 - CIPRA KH001/10425 study
Characteristics of tuberculosis ANRS 1295/12160 - CIPRA KH001/10425 study
SIGNIFICANT REDUCTION OF MORTALITY IN THE EARLY ARM * expressed in person-years ** per 100 person-years 12 patients (1.8%) lost to follow-up. 8,955 protocol visits, <2% missed visits. ANRS 1295/12160 - CIPRA KH001/10425 study
Kaplan-Meier survival curves Log-rank p-value: p=0.0042 ANRS 1295/12160 - CIPRA KH001/10425 study
Factors independently associated with mortality Cox proportional hazard model ANRS 1295/12160 - CIPRA KH001/10425 study * Also adjusted for site and CD4 level at baseline (stratification factors)
IRIS significantly more frequent in the early arm * expressed in person-months ** per 100 person-months Time after TB treatment initiation (weeks) ANRS 1295/12160 - CIPRA KH001/10425 study
>95% undetectable viral loadatweek 50 Plasma viral load (VL) measured by real time PCR for HIV-1 RNA plasmatic quantification (ANRS kit). ANRS 1295/12160 - CIPRA KH001/10425 study
CD4 increase from baseline Week 0: median CD4+ cell count was 25/mm3 Median CD4 increase at week 50: 114/mm3 ANRS 1295/12160 - CIPRA KH001/10425 study
CONCLUSIONS 1.Mortalitywasreduced by 34% when HAART wasinitiated 2 weeksvs. 8 weeksafteronset of TB treatment. 2. Irrespective of study arm, HAART has been extremelysuccessful, as evidenced by >95% of patients withundetectable viral load. 3.Despiteextremelylow CD4+ cell count at inclusion, patients enrolled in thispivotalstrategic trial have been extremelyadherent. 4. HAART initiation 2 weeksafteronset of TB treatmentcouldpotentiallysave 150,000 of the 450,000 annual HIV-TB deaths. ANRS 1295/12160 - CIPRA KH001/10425 study
ACKNOWLEDGEMENTS Sponsors: ANRS and NIH/DAIDS Cambodian Health Committee Institut Pasteur du Cambodge Médecins Sans Frontières – Belgium Cambodian Ministry of Health Cambodian National TB Program (CENAT) Cambodian National AIDS Program (NCHADS) Study sites: Khmer-Soviet Friendship Hospital (Phnom Penh), Donkeo Provincial Hospital (Takeo), Calmette Hospital (Phnom Penh), Svay Rieng Provincial Hospital and Siem Reap Referral Hospital Investigators, nurses, technicians, monitors, social workers… Members of the DSMB and the Scientific Advisory Board And especially all the patients and PLWHA representatives who joined us in this challenge. ANRS 1295/12160 - CIPRA KH001/10425 study