Download
1 / 1
20 likes | 499 Views
Improving Hand-Off Process between the Emergency Department (ED) and Inpatient Units (4B&5B) 5B Nursing Unit: Sara Bhullar, RN, Karla Jackson, RN, Julie Grunawalt, RN, MS, GCNS-BC , & Winnie Wood, MSN , RN , CNS 4B Nursing Unit: Jessie Rees , RN, Kim Ploegstra, RN

E N D
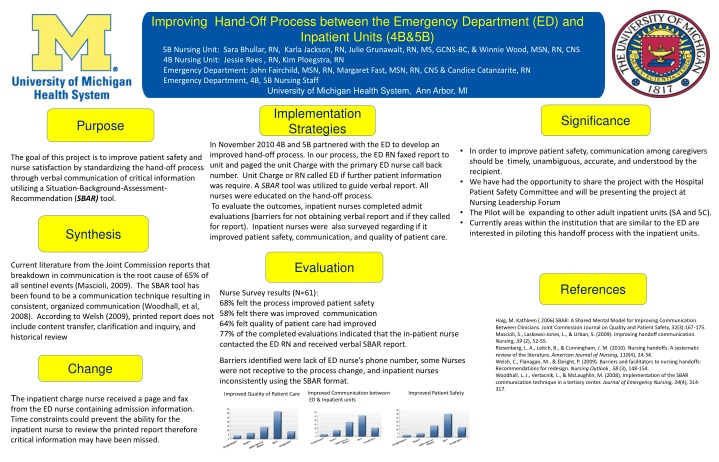
Improving Hand-Off Process between the Emergency Department (ED) and Inpatient Units (4B&5B) 5B Nursing Unit: Sara Bhullar, RN, Karla Jackson, RN, Julie Grunawalt, RN, MS, GCNS-BC, &Winnie Wood, MSN, RN, CNS 4B Nursing Unit: Jessie Rees , RN, Kim Ploegstra, RN Emergency Department: John Fairchild, MSN, RN, Margaret Fast, MSN, RN, CNS & Candice Catanzarite, RN Emergency Department, 4B, 5B Nursing Staff University of Michigan Health System, Ann Arbor, MI Significance Implementation Strategies Purpose In November 2010 4B and 5B partnered with the ED to develop an improved hand-off process. In our process, the ED RN faxed report to unit and paged the unit Charge with the primary ED nurse call back number. Unit Charge or RN called ED if further patient information was require. A SBAR tool was utilized to guide verbal report. All nurses were educated on the hand-off process. To evaluate the outcomes, inpatient nurses completed admit evaluations (barriers for not obtaining verbal report and if they called for report). Inpatient nurses were also surveyed regarding if it improved patient safety, communication, and quality of patient care. • In order to improve patient safety, communication among caregivers should be timely, unambiguous, accurate, and understood by the recipient. • We have had the opportunity to share the project with theHospital Patient Safety Committee and will be presenting the project at Nursing Leadership Forum • The Pilot will be expanding to other adult inpatient units (5A and 5C). • Currently areas within the institution that are similar to the ED are interested in piloting this handoff process with the inpatient units. The goal of this project is to improve patient safety and nurse satisfaction by standardizing the hand-off process through verbal communication of critical information utilizing a Situation-Background-Assessment-Recommendation (SBAR) tool. Synthesis Evaluation Current literature from the Joint Commission reports that breakdown in communication is the root cause of 65% of all sentinel events (Mascioli, 2009). The SBAR tool has been found to be a communication technique resulting in consistent, organized communication (Woodhall, et al, 2008). According to Welsh (2009), printed report does not include content transfer, clarification and inquiry, and historical review References Nurse Survey results (N=61): 68% felt the process improved patient safety 58% felt there was improved communication 64% felt quality of patient care had improved 77% of the completed evaluations indicated that the in-patient nurse contacted the ED RN and received verbal SBAR report. Barriers identified were lack of ED nurse’s phone number, some Nurses were not receptive to the process change, and inpatient nurses inconsistently using the SBAR format. Haig, M. Kathleen ( 2006) SBAR: A Shared Mental Model for Improving Communication Between Clinicians. Joint Commission Journal on Quality and Patient Safety, 32(3):167-175. Mascioli, S., Laskowsi-Jones, L., & Urban, S. (2009). Improving handoff communication.Nursing,39 (2), 52-55. Riesenberg, L. A., Leitch, B., & Cunningham, J. M. (2010). Nursing handoffs: A systematic review of the literature. American Journal of Nursing, 110(4), 24-34. Welsh, C., Flanagan, M., & Ebright, P. (2009). Barriers and facilitators to nursing handoffs: Recommendations for redesign. Nursing Outlook , 58 (3), 148-154. Woodhall, L. J., Vertacnik, L., & McLaughlin, M. (2008). Implementation of the SBAR communication technique in a tertiary center. Journal of Emergency Nursing, 34(4), 314-317. Change Improved Communication between ED & Inpatient units Improved Patient Safety Improved Quality of Patient Care The inpatient charge nurse received a page and fax from the ED nurse containing admission information. Time constraints could prevent the ability for the inpatient nurse to review the printed report therefore critical information may have been missed.