Download
1 / 64
660 likes | 720 Views
Explore the intricacies of thermoregulation in the human body, its mechanisms, and implications in anesthesia, including inadvertent hypothermia. Learn how to manage core temperature during medical procedures effectively.

E N D
Thermoregulation Hatice Türe, MD. Yeditepe University School of Medicine Department of Anesthesiology and Reanimation, İstanbul
Body Temperature • Shell temperature: • Temperature closer to skin • Oral temperature • 36.6o-37.0oC (97.9o-98.6oF) • Core temperature: • Most important temperature • Temperature of “core” (organs in cranial, thoracic and abdominal cavities) • Rectal temperature • 37.2o-37.6oC (99.0o-99.7oF)
Heat Production • Exergonic reactions: • Oxidation and ATP use. • Most heat generated by brain, heart, liver and glands at rest. • Skeletal muscles 20-30% at rest. Can increase 30-40 times during exercise.
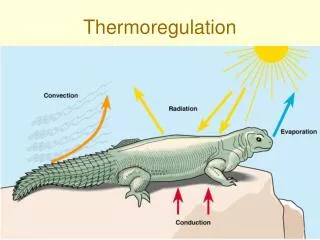
Mechanisms of Heat Transfer • Radiation: • Infrared radiation. • Conduction: • Direct transfer of energy through physical contact. • Convection: • Heat loss to air around the human body. • Evaporation: • Energy change in water molecule from liquid to vapor.
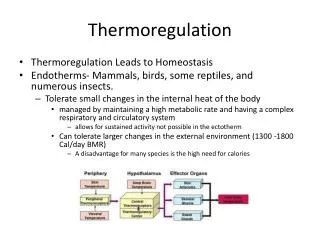
Normal thermoregulation • Processing of thermoregulatory information: afferent input central control efferent responses
Thermoregulatory Center • Hypothalamus: • Preoptic area neurons: hypothalamic thermostat: • Heat-losing center • Heat-promoting center • Monitors temperature of blood and receives signals from peripheral thermoreceptors. • Negative feedback loops
Heat-losing center: • Activates heat losing mechanisms: • Dilation of dermal arterioles: increase blood flow to skin. • Sweating. • Increased respiration through mouth. • Behavioral: remove clothing. • Inhibits heat-promoting center.
Heat-promoting center: • Activates heat generating mechanisms: • SNS: • Vasoconstriction of dermal arterioles: decrease blood flow to skin • Stimulates arrector pili muscles: hair stands on end • Shivering thermogenesis: spinal reflex of alternating contractions in antagonistic muscles • Nonshivering thermogenesis: • Long-term mechanism stimulating thyroid hormone release T3 and T4. • Inhibits heat-loss center.
Thermoregulatory Center • Hypothalamus: • Peripheral thermoreceptors: • Temperature of skin. • Central thermoreceptors: • Temperature of core. • Most important located in hypothalamus.
Core temperature measurements pulmonary artery tympanic membrane distal esophagus nasopharynx
Thermoregulation during general anesthesia • General anesthesia removes patient’s ability to regulate body temperature through behavior, so that autonomic defenses alone are available to respond to changes in temperature • Anesthetics inhibit thermoregulation in a dose-dependent manner and inhibit vasoconstriction and shivering about 2-3 times as they restrict sweating
The gain and maximal response intensity of sweating and vasodilation are well preserved when volatile anesthetics is given • However volatile anesthetics reduces the gain of AV-shunt vasoconstriction,without altering the maximal response intensity • Nonshivering thermogenesis dosen`t occur in anesthetized adults • General anesthesia decreases the shivering threshold far more than the vasoconstriction threshold
Inadvertent hypothermia during general anesthesia • Inadvertent hypothermia during general anesthesia is by far the most common perioperative thermal disturbance(due to impaired thermoregulation and cold environment). • Heat transferred from patient to environment: radiation > convection >>conduction & evaporation
Patterns of intraoperative hypothermia Phase I: Initial rapid decrease Phase II : Slow linear reduction Phase III: Thermal plateau
Initial rapid decrease • heat redistribution: decreases 0.5-1.5℃ during 1st hr • Tonic thermoregulatory vasoconstrictionthat maintains a temperature gradient between the core and periphery of 2-4℃ is broken • The loss of heat from the body to environment is little • Heat redistribution decreases core temperature, but mean body temperature and body heat content remain unchanged
2. Slow linear reduction • decreases in a slow linear fashion for 2-3hrs • Simply because heat loss >metabolic heat production • 90% heat loss through skin surface by radiation and convection
3. Thermal plateau • After 3-5 hrs,core temperature stops decreasing • It may simply reflect a steady state that heat loss=heat production in well-warmed p`t • If a p`t is sufficiently hypothermic,plateau phase means activation of vasoconstriction to reestablish the normal core-to-peripheral temperature gradient • Temperature plateau due to vasoconstriction is not a thermal steady state and body heat content continues to decrease even though temperature remains constant
Regional Anesthesia • Regional anesthesia impairs both central and peripheral thermoregulation • Hypothermia is common in patients given spinal or epidural anesthetics
The human thermoregulatory system usually maintains core body temperature within 0.2℃ of 37℃ • Perioperative hypothermia is common because of the inhibition of thermoregulation induced by anesthesia and the patient`s exposure to cool enviroment • Hypothermia complication: Shivering,prolonged drug effect,coagulopathy, surgical wound infection,morbid cardiac event
Hypothermia • Core temperature below 95oF (350). • Gradual loss of mental and physical activity. • Changes in motor coordination. • Shivering. • Slurred speech. • Abnormally slow rate of breathing. • Cold, pale skin. • Fatigue, lethargy.
If core temperature remains above 90oF (32o) recovery is good. • If core temperature falls below 80o F, (27o) prognosis poor. • Treatment: • Move person out of cold. • Insulate the person’s body. • Warm beverages. • Give warm IV fluids, slowly otherwise vasodilation occurs, bringing too large volume of chilled blood; cardiac arrhythmias. • Frostbite: • Vasoconstriction to cold, causes irreparable tissue damage. • Cells decrease ATP production, hypoxia. • Do not rub tissue.
Undetected hypothermia • The core temperature is rarely monitored by medical personnel during spinal and epidural anesthesia • Patients usually do not feel cold
Heat Balance and Shivering Initial hypothermia (Phase I) • Redistribution of heat from core to periphery • Primarily caused by peripheral inhibition of tonic thermoregulatory vasoconstriction • Although the vasodilatation of AV shunts is restricted to the lower body, the mass of the legs is sufficient to produce substantial core hypothermia
Subsequent hypothermia (Phase II) • Loss of heat exceeds production • Patients given SA or EA cannot reestablish core-temperature equilibrium because peripheral vasoconstriction remains impaired • Hypothermia tends to progress throughout surgery
Shivering • Occurs during spinal and epidural anesthesia • Disturb patients and care givers but produced relatively little heat because it is restricted to the small-muscle mass cephaled to the block • Treated by warming surface of skin or administration of clonidine / meperidine
Consequences of Hypothermia Advantages • Provide substantial protection against cerebral ischemia and hypoxia • Slows the triggering of malignant hyperthermia and reduce its severity • Appear to facilitate recovery and reduce mortality from septic ARDS
Disadvantages • Wound infection---the most common serious complication, due to • Impaired immune function • decreased cutaneous blood flow • protein wasting • decreased synthesis of collagen
Metabolic effects • Increased oxygen consumption and decreased CO2 production • Increased haemoconcentration, hypoxia, metabolic acidosis • Liver and renal dysfunction • Metabolic inhibition (heparin, citrat, lactic acide) • CNS depression, pupiller midriasis and EEG depression (under 300), consciousness (under 280), death (under 210)
Metabolic effects • GFR (poliuria, oliguria, anuria) • Hyperglisemia • Htc
Coagulopathy • Hypothermia reduces platelet function and decreases the activation of the coagulation cascade • From in vitro studies, it increased the loss of blood and the need for allogenic transfusion during elective primary hip arthroplasty • Just 1.5 ℃ of core hypothermia triples the incidence of VT and morbid cardiac events
Drug metabolism • Mild hypothermia decreases the metabolism of most drugs • Propofol ---during constant infusion, plasma conc. is 30 percent greater than normal • Atracurium---a 3 ℃ reduction in core temp. increase the duration of muscle relaxation by 60 percent • Significantly prolongs the postoperative recovery period
Thermal comfort • Patients feel cold in postoperative period, sometimes rating it worse than surgical pain • Shivering occurs in ~40% of unwarmed patients who recovers from GA
Treating and Preventing Intraoperative Hypothermia Preventing redistribution hypothermia • The initial reduction in core temperature is difficult to treat because it result from redistribution of heat • Prevent by skin-surface warming • Peripheral heat content ↑ → Temperature gradient ↓ → Redistribution of heat ↓
Airway heating and humidification • Less than 10% of metabolic heat is lost through respiratory • Two thirds of heat in humidifying inspiratory gases • Passive or active airway heating and humidification contribute little to thermal management
Intravenous fluids • 1L of IV fluids at ambient temperature or 1 unit of refrigerated blood decreases the mean body temperature 0.25 ℃ • Heating fluids to near 37 ℃ helps prevent hypothermia and is appropriate if large volumes are being given
Cutaneous Warming • The skin is the predominant source of heat loss during surgery, mostly by radiation and convection • Evaporation from large surgical incisions may be important • An ambient temp. above 25℃ is frequently required, but this is uncomfortable for gowned surgeons
Heat loss can be reduced by covering the skin( with surgical draps, blankets, or plastic bags……) • Insulator • Forced-air warming • Typically, forced-air warming alone or combined with fluid warming is required to maintain normal intraoperative core temp.
Elevation of core body temperature above the normal diurnal range of 36ºC to 37.5ºC due to failure of thermoregulation • Hyperthermia is not synonymous with the more common sign of fever, which is induced by cytokine activation during inflammation, and regulated at the level of the hypothalamus
The most important causes of severe hyperthermia (greater than 40ºC or 104ºF) caused by failure of thermoregulation are: • Heat stroke • Neuroleptic malignant syndrome • Malignant hyperthermia
Physiology • Body temperature is maintained within a narrow range by balancing heat load with heat dissipation. • Body's heat load results from both metabolic processes and absorption of heat from the environment • As core temperature rises, the preoptic nucleus of the anterior hypothalamus stimulates efferent fibers of the ANS to produce sweating and cutaneous vasodilation.
Evaporation is the principal mechanism of heat loss in a hot environment, but this becomes ineffective above a relative humidity of 75% • Other methods of heat dissipation • Radiation- emission of infrared electromagnetic energy • Conduction- direct transfer of heat to an adjacent, cooler object • Convection-direct transfer of heat to convective air currents • These methods cannot efficiently transfer heat when environmental temperature exceeds skin temperature.
Temperature elevation ↑ O2 consumption and metabolic rate hyperpnea and tachycardia • Above 42ºC (108ºF), oxidative phosphorylation becomes uncoupled, and a variety of enzymes cease to function. • Hepatocytes, vascular endothelium, and neural tissue are most sensitive to these effects, but all organs may be involved. • As a result, these patients are at risk of multiorgan system failure.
Heat Stroke • Core body temperature > 40.5ºC (105ºF) with associated CNS dysfunction in the setting of a large environmental heat load that cannot be dissipated • Complications include: • ARDS • DIC • Renal or hepatic failure • Hypoglycemia • Rhabdomyolysis • Seizures
Classic (nonexertional) heat stroke • Affects individuals with underlying chronic medical conditions that either impair thermoregulation or prevent removal from a hot environment. • Conditions include: • Cardiovascular disease • Neurologic or psychiatric disorders • Obesity • Anhidrosis • Extremes of age • Anticholinergic agents or diuretics
Exertional heat stroke • Occurs in young, otherwise healthy individuals engaged in heavy exercise during periods of high ambient temperature and humidity • Findings include cutaneous vasodilation, tachypnea, rales due to noncardiogenic pulmonary edema, excessive bleeding due to DIC, altered mentation or seizures • Labs: coagulopathy, ARF, elevated LFTs due to acute hepatic necrosis, respiratory alkalosis, and aleukocytosis as high as 30,000-40,000/mm3
Malignant Hyperthermia • Rare genetic disorder manifests after tx with anesthetic agents: succinylcholine and halothane • Onset is usually in 1 hour of the administration of anesthesia, rarely delayed up to 10 hours • ½ of cases are inherited in as AD; Rest are inherited in different patterns. • Susceptible patients with AD disease have any one of several distinct mutations in the gene for the SKM ryanodine receptor (RyR1) which is a homotetrameric Ca++ channel in the sarcoplasmic reticulum of SKM • In the presence of anesthetic agents, alterations in the hydrophilic, amino-terminal portion of the ryanodine receptor uncontrolled Ca ++ efflux from the SR tetany,↑ SKM metabolism, and heat production • For unclear reasons, overexpression of the wild-type ryanodine receptor does not ablate abnormal myocyte responses to halothane although overexpression of a mutated ryanodine receptor can induce the malignant hyperthermia phenotype in myocytes from normal individuals
Malignant Hyperthermia • Early clinical findings in malignant hyperthermia include muscle rigidity (especially masseter stiffness), sinus tachycardia, increased CO2 production, and skin cyanosis with mottling • Marked hyperthermia (up to 45ºC [113ºF]) occurs minutes to hours later; core body temperature tends to rise 1ºC every 5 to 60 minutes. • Hypotension, complex dysrhythmias, rhabdomyolysis, electrolyte abnormalities, DIC and mixed acidosis accompany the elevated temperature. • Rarely, biochemically-proven malignant hyperthermia may present solely with rhabdomyolysis in the absence of hyperthermia