Download
1 / 1
10 likes | 311 Views
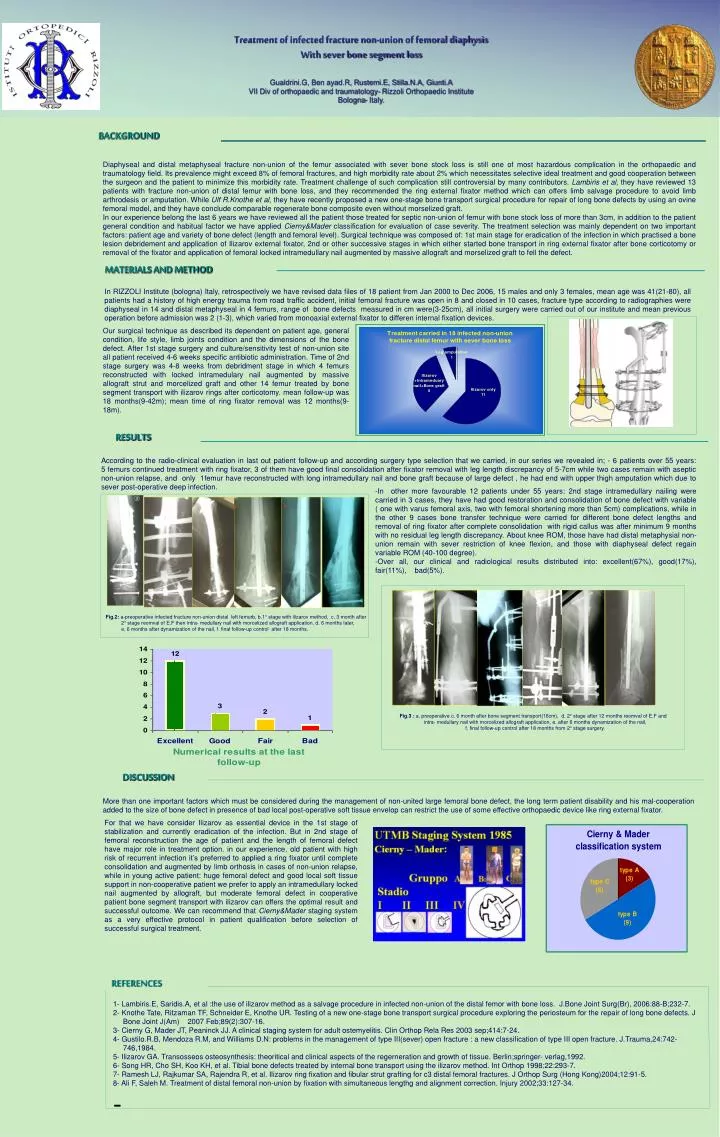
MATERIALS AND METHOD. RESULTS. DISCUSSION. Treatment of infected fracture non-union of femoral diaphysis With sever bone segment loss Gualdrini.G, Ben ayad.R, Rustemi.E, Stilla.N.A, Giunti.A VII Div of orthopaedic and traumatology- Rizzoli Orthopaedic Institute Bologna- Italy.

E N D
MATERIALS AND METHOD RESULTS DISCUSSION Treatment of infected fracture non-union of femoral diaphysis With sever bone segment loss Gualdrini.G, Ben ayad.R, Rustemi.E, Stilla.N.A, Giunti.A VII Div of orthopaedic and traumatology- Rizzoli Orthopaedic Institute Bologna- Italy. BACKGROUND Diaphyseal and distal metaphyseal fracture non-union of the femur associated with sever bone stock loss is still one of most hazardous complication in the orthopaedic and traumatology field. Its prevalence might exceed 8% of femoral fractures, and high morbidity rate about 2% which necessitates selective ideal treatment and good cooperation between the surgeon and the patient to minimize this morbidity rate. Treatment challenge of such complication still controversial by many contributors. Lambiris et al, they have reviewed 13 patients with fracture non-union of distal femur with bone loss, and they recommended the ring external fixator method which can offers limb salvage procedure to avoid limb arthrodesis or amputation. While UlfR.Knothe et al, they have recently proposed a new one-stage bone transport surgical procedure for repair of long bone defects by using an ovine femoral model, and they have conclude comparable regenerate bone composite even without morselized graft. In our experience belong the last 6 years we have reviewed all the patient those treated for septic non-union of femur with bone stock loss of more than 3cm, in addition to the patient general condition and habitual factor we have applied Cierny&Mader classification for evaluation of case severity. The treatment selection was mainly dependent on two important factors: patient age and variety of bone defect (length and femoral level). Surgical technique was composed of: 1st main stage for eradication of the infection in which practised a bone lesion debridement and application of Ilizarov external fixator, 2nd or other successive stages in which either started bone transport in ring external fixator after bone corticotomy or removal of the fixator and application of femoral locked intramedullary nail augmented by massive allograft and morselized graft to fell the defect. In RIZZOLI Institute (bologna) Italy, retrospectively we have revised data files of 18 patient from Jan 2000 to Dec 2006, 15 males and only 3 females, mean age was 41(21-80), all patients had a history of high energy trauma from road traffic accident, initial femoral fracture was open in 8 and closed in 10 cases, fracture type according to radiographies were diaphyseal in 14 and distal metaphyseal in 4 femurs, range of bone defects measured in cm were(3-25cm), all initial surgery were carried out of our institute and mean previous operation before admission was 2 (1-3), which varied from monoaxial external fixator to differen internal fixation devices. Our surgical technique as described its dependent on patient age, general condition, life style, limb joints condition and the dimensions of the bone defect. After 1st stage surgery and culture/sensitivity test of non-union site all patient received 4-6 weeks specific antibiotic administration. Time of 2nd stage surgery was 4-8 weeks from debridment stage in which 4 femurs reconstructed with locked intramedulary nail augmented by massive allograft strut and morcelized graft and other 14 femur treated by bone segment transport with ilizarov rings after corticotomy. mean follow-up was 18 months(9-42m); mean time of ring fixator removal was 12 months(9-18m). According to the radio-clinical evaluation in last out patient follow-up and according surgery type selection that we carried, in our series we revealed in; - 6 patients over 55 years: 5 femurs continued treatment with ring fixator, 3 of them have good final consolidation after fixator removal with leg length discrepancy of 5-7cm while two cases remain with aseptic non-union relapse, and only 1femur have reconstructed with long intramedullary nail and bone graft because of large defect , he had end with upper thigh amputation which due to sever post-operative deep infection. • In other more favourable 12 patients under 55 years: 2nd stage intramedullary nailing were carried in 3 cases, they have had good restoration and consolidation of bone defect with variable ( one with varus femoral axis, two with femoral shortening more than 5cm) complications, while in the other 9 cases bone transfer technique were carried for different bone defect lengths and removal of ring fixator after complete consolidation with rigid callus was after minimum 9 months with no residual leg length discrepancy. About knee ROM, those have had distal metaphysial non-union remain with sever restriction of knee flexion, and those with diaphyseal defect regain variable ROM (40-100 degree). • Over all, our clinical and radiological results distributed into: excellent(67%), good(17%), fair(11%), bad(5%). Fig.2: a-preoperative infected fracture non-union distal left femurb, b.1° stage with ilizarov method, c. 3 month after 2° stage reomval of E.F then intra- medullary nail with morcelized allograft application, d. 6 months later, e. 6 months after dynamization of the nail, f. final follow-up control after 18 months. e f d d e Fig.3 : a. preoperative c. 6 month after bone segment transport(16cm), d. 2° stage after 12 months reomval of E.F and intra- medullary nail with morcelized allograft application, e. after 6 months dynamization of the nail, f. final follow-up control after 18 months from 2° stage surgery. More than one important factors which must be considered during the management of non-united large femoral bone defect, the long term patient disability and his mal-cooperation added to the size of bone defect in presence of bad local post-operative soft tissue envelop can restrict the use of some effective orthopaedic device like ring external fixator. For that we have consider Ilizarov as essential device in the 1st stage of stabilization and currently eradication of the infection. But in 2nd stage of femoral reconstruction the age of patient and the length of femoral defect have major role in treatment option. in our experience, old patient with high risk of recurrent infection it’s preferred to applied a ring fixator until complete consolidation and augmented by limb orthosis in cases of non-union relapse, while in young active patient: huge femoral defect and good local soft tissue support in non-cooperative patient we prefer to apply an intramedullary locked nail augmented by allograft, but moderate femoral defect in cooperative patient bone segment transport with ilizarov can offers the optimal result and successful outcome. We can recommend that Cierny&Mader staging system as a very effective protocol in patient qualification before selection of successful surgical treatment. REFERENCES • 1- Lambiris.E, Saridis.A, et al :the use of ilizarov method as a salvage procedure in infected non-union of the distal femor with bone loss. J.Bone Joint Surg(Br), 2006:88-B;232-7. • 2- Knothe Tate, Ritzaman TF, Schneider E, Knothe UR. Testing of a new one-stage bone transport surgical procedure exploring the periosteum for the repair of long bone defects. J Bone Joint J(Am) 2007 Feb;89(2):307-16. • 3- Cierny G, Mader JT, Peaninck JJ. A clinical staging system for adult ostemyelitis. Clin Orthop Rela Res 2003 sep;414:7-24. • 4- Gustilo.R.B, Mendoza R.M, and Williams D.N: problems in the management of type III(sever) open fracture : a new classification of type III open fracture. J.Trauma,24:742-746,1984. • 5- Ilizarov GA. Transosseos osteosynthesis: theoritical and clinical aspects of the regerneration and growth of tissue. Berlin;springer- verlag,1992. • 6- Song HR, Cho SH, Koo KH, et al. Tibial bone defects treated by internal bone transport using the ilizarov method. Int Orthop 1998;22:293-7. • 7- Ramesh LJ, Rajkumar SA, Rajendra R, et al. Ilizarov ring fixation and fibular strut grafting for c3 distal femoral fractures. J Orthop Surg (Hong Kong)2004;12:91-5. • 8- Ali F, Saleh M. Treatment of distal femoral non-union by fixation with simultaneous lengthg and alignment correction. Injury 2002;33:127-34.