Download

1 / 10
110 likes | 172 Views
Learn why implementing best practices in trichiasis surgery is crucial to reduce blindness and disability. Discover potential solutions for training, supervision, and surgery delivery to enhance outcomes and reach elimination goals through evidence-based actions.

E N D
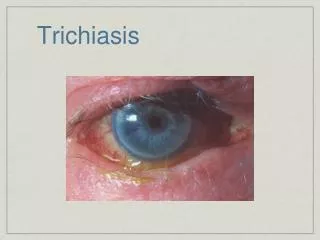
Why do we need “best practices” for trichiasis surgery? • Trichiasis continues to be a major cause of blindness & disability • Surgeries considerably fewer than needed to eliminate backlog • Quality of outcomes not as good as needed • Research carried out in the past few years provides evidence for improvements to: • Surgery itself • Training and supervision • Programmatic approaches
Defining a “best practice”: Philosophic approaches Best practice: • Efficient • Effective Philosophic approach: • Patient centered care • Quality of service important • Evidence needed to guide actions • Health systems need strengthening
Improving surgery Problems: • Considerable variation in TT surgical outcome • Poor outcome often high • Some patients need follow up surgery • Evidence suggests outcome could be improved
Improving surgery Potential solutions: • Post op follow up within 6 mo. • Improve training (short incision length associated with post operative TT) • Certification (need to follow Final Assessment Manual) • Maintain sterility • Management of recurrence should be tailored to clinical features & patient needs
Can we improve the surgery training? Problems: • Attrition of TT surgeons often high • Dedicated eye workers doing most surgery Potential solutions: • Selection of trainees needs clear criteria (including binocular vision & manual dexterity) • Train/use more dedicated eye workers • Develop training of trainers manual
Supervision of TT surgeons Problems: • Minimal supervision in place • Outcome rarely reported Potential solutions: • Include supportive supervision as part of HSS • Identify surgeon supervisor as team leader (training needed) • Develop supervision guidelines
Are we going to meet our TT targets? Problems: • At current productivity levels 28 yrs needed to address existing backlog • Campaign/outreach often account for 65-85% of total surgeries • Static service alone insufficient (current approaches to train and deploy general health workers insufficient)
Are we going to meet our TT targets? Potential solutions: • Campaign/outreach needed • Will require additional dedicated eye care personnel • Manual on how to conduct efficient/effective outreach needed
Summary • All aspects of trichiasis surgical service delivery needs revision • Selection of surgeons • Training of surgeons • Mobilization • Outreach • Use evidence to guide actions • Reaching elimination possible