Download
1 / 34
370 likes | 680 Views
Red Blood Cells & Anemias. RBC: ~5 x 10 6 / m l; Generate ~ 8,000,000,000/hour. Andrew D. Leavitt, MD Departments of Laboratory Medicine & Medicine. March 26, 2012. Outline – topics we will cover. Erythropoiesis – names, faces, & numbers (review) RBC biology - Hemoglobin

E N D
Red Blood Cells & Anemias RBC: ~5 x 106/ml; Generate ~ 8,000,000,000/hour Andrew D. Leavitt, MD Departments of Laboratory Medicine & Medicine March 26, 2012
Outline – topics we will cover • Erythropoiesis – names, faces, & numbers (review) • RBC biology - Hemoglobin • O2 dissociation curves • Hemoglobin – fetal, adult • RBC membrane • Hemoglobin switching • Anemias: Production vs. destruction vs. loss • Membrane or contents – Hgb, enzymes • Immune mediated • Physical destruction • Anemia of inflammation • Ribosomopathies
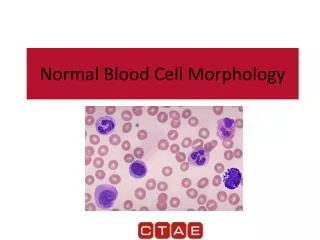
Pro- Erythroblast Basophilic Erythroblast Polychromatic Erythroblast Orthochromatic Erythroblast RBC Reticulocyte 5 stages in the marrow Erythropoiesis CHROMATIN STRUCTURE NUCLEAR SIZE & COLOR CELL SIZE & CYTOPLASM COLOR Abbott Labs, Morphology of Human Blood Cells
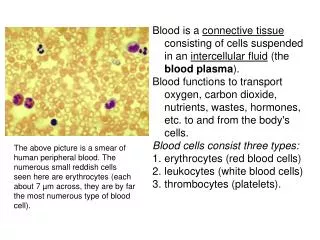
Red Blood Cell (RBC) Delivers O2 from your lungs to all your tissues Takes CO2 from your tissues to your lungs Also – binds NO (a vasodilator) Their size: 8 [capillaries have ~3 M diameter] Their life-span: 120 days Mature RBCs have no nucleus Too few RBCs = anemia
What tells your body to make RBCs? EPO: Is not stored, but expressed in response to the kidney sensing oxygen in the blood It - 1. Increases # of E-committed progenitors 2. Increase GATA1 and FOG expression 3. Enhances anti-apoptotic gene expression 4. Increases transferrin receptor expression
Hemoglobin Hemoglobin (Hgb) in the RBC carries O2, which is poorly soluble in water, to tissues & CO2 from tissues to lungs. ~640,000,000 Hemoglobin molecules/RBC Must coordinate: 1.heme and globin synthesis 2. a (Chromosome 11; 141 aa) & b (Chromnosome 16; 146) chains Colors of a bruise are globin breakdown products Heme Iron in a Porphyrin ring b6Gluto Val Tetramer of two heterodimers (a &b) Linus Pauling 1949 – molecular diagnosis 2012 – no therapy
Hemoglobin oxygen dissociation curve Mean Venous O2 tension Arterial O2 tension HbF ; CO2
a a 50 g b Globin chain synthesis (%) e z d 0 Adult Embryo Fetus Birth 6 mo. HgA a2b2 (96-98) HgA2a2d2 (2-3) HgF a2g2 (< 1) HgF a2g2 (75) HgA a2b2 (25) Erythropoiesis: Hemoglobin Switching(ALWAYS: 2 alpha & 2 “beta-like” [3 ‘b’ options]) Alpha: Chromosome 16 Beta-like: Chromosome 11 Hoffman et al. Hematology 2000
Schematic of red cell membrane depicting proteins crucial for normal membrane mechanical strength * * *mutations lead to hereditary spherocytosis
Thinking about anemia…a clinical perspective Framework: RBC size (MCV) & is the marrow responding (reticulocyte count) Etiology: Cell intrinsic: 1. Hgb – too little; abnormal type; unequal a and b synthesis 2. Enzyme 3. Membrane Cell extrinsic: Immune mediated Physical destruction Blood loss Marrow does not produce Primary – leukemia, myelodysplasia Secondary – vitamin deficiency
Reticulocyte Stain – detects the ribonucleoprotein in the young RBC Reticulocytes
#1.1 Too little Hgb: Iron Deficiency Anemia Small cells – microcytic (MCV < 80 fL) Young women – OK Older people – Worry about gastrointestinal blood loss Iron deficiency anemia, peripheral blood (40x) normal peripheral blood (40x) Lead poisoning can look like Fe deficiency – Lead blocks heme synthesis
peripheral blood, 100X Iron Deficiency Anemia Iron stian of bone marrow – none found Elliptocytes Hypochromic RBCs ~ 500 million people worldwide
The Iron Circuit – mostly a game of recycling Daily absorption: Duodenum ~ 1 mg Daily loss: urine, feces, skin, hair ~ 1 mg Transferrin Plasma (4 mg) Ineffective erythropoiesis Macrophage (0.5 – 1.5 gm) Bone Marrow Erythroblasts ( ~ 150 mg) Circulating RBCs (1.7 – 2.4 gm) Menstrual loss/hemorrhage
Iron Circuit in Disease Infection/inflammation/malignancy IL-6/LPS hepcidin (25aa protein) absorption macrophage Fe storage Impairs Erythropoiesis: Decrease EPO Directly suppresses marrow Interferon – g TNF – a IL-1, IL-10 Weiss & Goodnough NEJM 2005
Iron stain of bone marrow aspirates Iron deficienyc anemia - iron stain Storage iron (blue) Anemia of inflammation – iron stain
#1.2 Abnormal Hgb: Sickle cell disease Multi-system disease Cardiovascular/strokes Kidneys Skin Lungs Immune system Treatment: Supportive care Transfusions Demethylating agents Stem cell transplants
#1.3 Abnormal a/b Globin ratio: Thalassemia Small cells – microcytic (MCV < 80 fL) Imbalance between a and b chains Name based on which chain is deficient [a or b thal] Make lots of RBCs, just unstable and lyse, so increased retics Alpha Thal: silent carrier -a / aa trait -- / aa or -a / -a Hgb H -a / -- Hydrops fetalis -- /-- Beta Thal: Minor Intermedia Major
a a 50 g b Globin chain synthesis (%) e z d 0 Adult Embryo Fetus Birth 6 mo. HgA a2b2 (96-98) HgA2a2d2 (2-3) HgF a2g2 (< 1) HgF a2g2 (75) HgA a2b2 (25) Erythropoiesis: Hemoglobin Switching(ALWAYS: 2 alpha & 2 “beta-like” [3 ‘b’ options]) Alpha: Chromosome 16 Beta-like: Chromosome 11 Hoffman et al. Hematology 2000
Normal peripheral smear Alpha thal trait Hemoglobin H, -- / -A Beta-thalassemia major Target cells Nucleated RBC Target cells Retics
Beta-thalassemia major (transfused) Severe thalassemia Beta-thalassemia major Target cells Normal RBCs (transfused) Nucleated RBC Nucleated RBC
Arrows show Heinz bodies #2 Enzyme: G-6-PD deficiency (Heinz body hemolytic anemia) Reduced glutathione (GSH) is critical for RBCs to counter oxidative stress. Bite cells Sulfa drugs, fava beans, antimalarials..…
#3: Membrane: red cell membrane depicting proteins crucial for normal membrane mechanical strength * * *mutations lead to hereditary spherocytosis
Hereditary spherocytosis (HS) Reticulocytes spherocytes
Thinking about anemia…a clinical perspective Framework: RBC size (MCV) & is the marrow responding (reticulocyte count) Etiology: Cell intrinsic: 1. Hgb – too little; abnormal type; unequal a and b synthesis 2. Enzyme 3. Membrane Cell extrinsic: Immune mediated Physical destruction Blood loss Marrow does not produce Primary – leukemia, myelodysplasia Secondary – vitamin deficiency
Autoimmune hemolytic anemia Reticulocytes spherocytes
Testing for anti-RBC antibodies: attached or in circulation Hemolytic disease of the newborn
RBC destruction - extrinsic Erythroid Hyperplasia, TTP, bone marrow aspirate (100x) Thrombotic thrombocytopenic purpura (TTP) schistocytes (RBC fragments) Hemolytic uremic syndrome (HUS) schistocytes (RBC fragments) Retics
Megaloblastic anemia (MCV > 100) B12 deficiency Folate deficiency Affects DNA synthesis
Megaloblastic anemia (MCV > 100) Anemia yet hypercellular marrow – ineffective erythropoiesis
Ribosomopathies and hematopoietic disorders Our findings indicate that the erythroid lineage has a low threshold for the induction of p53, providing a basis for the failure of erythro- poiesis in the 5q- syndrome, DBA, and perhaps other bone marrow failure syn- dromes. Narla & Ebert 2010
Take home message…… Blood is good…everyone should have some! Share it…become a blood donor if you can UCSF Blood donor center: Millberry Union next to Subway sandwich shop The best donor center nurses in town