Download
1 / 29
290 likes | 962 Views
Temporal Bone Fractures and Surgical Approaches for CSF Leaks. Arthur Wu, MD UCLA Division of Head and Neck Surgery. Incidence and Epidemiology. Blunt head trauma typically MVA Penetrating trauma eg. GSW have worse prognosis 2/2 carotid or brain injury. Symptoms.

E N D
Temporal Bone Fractures and Surgical Approaches for CSF Leaks Arthur Wu, MD UCLA Division of Head and Neck Surgery
Incidence and Epidemiology • Blunt head trauma typically MVA • Penetrating trauma eg. GSW have worse prognosis 2/2 carotid or brain injury
Symptoms • Hearing loss: conductive or sensorineural • Dizziness • Facial weakness or paralysis (7% overall) • Otorrhea • Rhinorrhea • More rare: facial numbness and diplopia
Physical Examination • Hemotympanum • Battle’s sign: postauricular ecchymosis • Raccoon sign: periorbital ecchymosis
Otoscopy • Otorrhea: bloody or clear and pulsatile (send for β2 transferrin) • Pneumatic otoscopy: vertigo or flaccid TM • Laceration of canal wall
Others • Nasal exam for rhinorrhea • Facial nerve exam • Extraocular movement exam for nystagmus or diplopia • Tuning fork exam • Audiometric testing
Imaging • High resolution CT is the gold standard • MRI for cranial nerve injury • MRA or angiogram for vascular injury
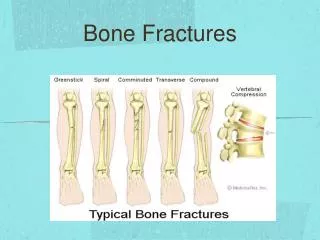
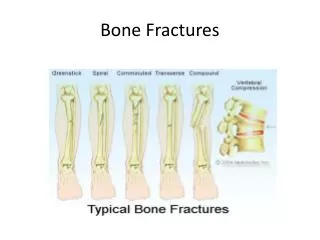
Types of fractures • Longitudinal: along long axis of the petrous temporal bone • Tranverse: perpendicular to the long axis of the petrous bone (commonly from the jugular foramen or foramen magnum to the middle cranial fossa) • Mixed: in reality most fractures are mixed type
Longitudinal Fractures • Most common (up to 80%) • Path of least resistance • Ossicular chain and the perigeniculate ganglion region of the facial nerve can be involved • Otic capsule involvement is rare • Facial nerve injury in 10-20%
Transverse Fractures • Commonly involves bony labrynth leading to SNHL and vertigo • Facial nerve injury quoted as up to 50% • Higher impact injuries • Anterior-Posterior force
The Good News • For vast majority of temporal bone fractures, we do nothing!
Indications for Surgical Intervention • Facial nerve injury • Hearing loss • CSF leak
Facial Nerve Injury • Overall 7% of temporal bone fractures, 25% of these being permanent • Delayed onset vs Immediate onset • Delayed onset: complete recovery in 94% • Immediate onset: complete recovery in 50-75% • Site of injury: 80-90% perigeniculate ie tympanic segment (followed by labrynthine and meatal)
Facial Nerve Injury • Goal: to explore only those nerves with crush injury or some degree of transection • Neuropraxia: Transient block of axoplasmic flow ( no neural atrophy/damage) • Axonotmesis: damage to nerve axon with preservation of the epineurium (regrowth) • Neurotmesis: Complete disruption of the nerve ( no chance of organized regrowth)
Nerve Conduction Testing • EMG and ENOG • If EMG shows voluntary activity, then good prognosis • EMG will show fibrillation potentials if nerve out in 2 wks (not very helpful) • Operate when ENOG shows 90% degeneration • Wallerian degeneration is not documented on electrodiagnostic testing for 3 to 5 days after the neurotmesis, surgical intervention is delayed until several days after the nerve has degenerated • The efficacy of decompression of a posttraumatic, nonsevered nerve remains to be proven in a randomized, prospective study • Note: ENOG requires normal side for comparison
Hearing Loss • 80% of conductive hearing loss resolves spontaneously • SNHL worse prognosis of recovery • If persistent CHL, then can take later to OR for possible ossicular reconstruction or tympanoplasty depending on etiology
CSF Leak • Otorrhea, rhinorrhea, dizziness, serous effusion, meningitis • 15-20% of all temporal bone fractures • Usually associated with longitudinal fractures involving the tegmen • High resolution CT usually sufficient; CT cisternogram may be helpful for specific site • Typically involves tear in dura of tegmen • Leaks 2/2 otic capsule disruption less likely to heal spontaneously
Conservative Treatment • HOB elevation > 30 deg • Lumbar drain • Stool softeners • No noseblowing, coughing • Brodie and Thompson et al. • 820 T-bone fractures/122 CSF leaks • Spontaneous resolution with conservative measures • 95/122 (78%): within 7 days • 21/122(17%): between 7-14 days • 5/122(4%): Persisted beyond 2 weeks
Preventing Meningitis: Antibiotics?? • Same study: 7% developed meningitis with no significant difference between those treated with antibiotics and not • Many studies demonstrate no benefit but difficult to see differences from overall low numbers • Hoff et al conducted a prospective randomized trial; no patients in either arm got meningitis • Metaanalysis by Brodie demonstrates difference of 8% vs 2% for abx vs no abx
Surgical Intervention From Cummings
Technique • Meta-analysis showed that both techniques have similar success rates • Onlay: if adjacent structures at risk, or if the underlay is not possible
Technique • Muscle, fascia, fat, cartilage, Duragen, bone pate, hydroxyapatite cement • The success rate is significantly higher for those patients who undergo primary closure with a multi-layer technique versus those patients who only get single-layer closure. • Refractory cases may require closure of the EAC and obliteration.
Leaks of the Lateral Tegmen • Accessed through transmastoid Taken from Myers
Leaks of the Medial Tegmen • May require transmastoid combined with middle fossa approach
References • Bailey, Byron J., ed. Head and Neck surgery- Otolaryngology. Philadelphia, P.A. J.B. Lippincott Co., 1993. • Cummings, ed. Otolaryngology: Head and Neck Surgery. 4th edition. • Brodie, HA, Thompson TC. Management of Complications from 820 Temporal Bone Fractures. American Journal of Otology; 18: 188-197, 1997. • Brodie HA, Prophylactic Antibiotic for Posttraumatic CSF Fistulas. Arch of Otolaryngology- Head and Neck Surgery; 123; 749-752, 1997. • Black, et al. Surgical Management of Perilymphatic Fistulas: A Portland experience. American Journal of Otology; 3: 254-261, 1992. • Chang CY, Cass SP. Management of Facial Nerve Injury Due to Temporal Bone Trauma. The American Journal of Otology; 20: 96-114, 1999. • Coker N, Traumatic Intratemporal Facial Nerve Injuries: Management Rationale for Preservation of Function. Otolaryngology- Head and Neck Surgery; 97:262-269, 1987. • Green, JD. Surgical Management of Iatrogenic Facial Nerve Injuries. Otolaryngolgoy- Head and Neck Surgery; 111; 606-610, 1994. • Lambert PR, Brackman DE. Facial Paralysis in Longitudinal Temporal Bone Fractures : A Review of 26 cases. Laryngoscope; 94:1022-1026, 1984. • Lee D, Honrado C, Har-El G. Pediatric Temporal Bone Fractures. Laryngoscope: vol 108(6). June 1998, p816-821. • Mckennan KX, Chole RA. Facial Paralysis in Temporal Bone Trauma. American Journal of Otology; 13: 354-261, 1982. • Savva A, Taylor M, Beatty C. Management of Cerebrospinal Fluid Leaks involving the Temporal Bone: Report on 92 Patients. Laryngoscope: vol 113(1). January 2003, p50-56 • Thaler E, Bruney F, Kennedy D, et al. Use of an Electronic Nose to Distinguish Cerebrospinal Fluid from Serum. Archives of Otolaryngology; vol 126(1). Jan 2000, p71-74.