Download

1 / 228
2.29k likes | 2.92k Views
GENITO URINARY SYSTEM. OBJECTIVES. At the end of the class students will be able to explain glomerulonephritis and its management enlist the congenital anomalies list down the features of renal failure explain nephrotic syndrome e numerate UTI. HELLO K I D N E Y.

E N D
OBJECTIVES At the end of the class students will be able to • explain glomerulonephritis and its management • enlist the congenital anomalies • list down the features of renal failure • explain nephrotic syndrome • enumerate UTI
HELLO K I D N E Y G l o m e r u l o n e p h r I t I s
What is glomerulonephritis? • Glomerulonephritis is is a kidney condition that involves damage /inflammation to the glomeruli.
Incidence and etiology • More in males • Between 5-8yrs • Peak age 7yrs • Beta Hemolytic streptococcus • Primary site or infection is usually the throat or skin after nephritis.
Types of glomerulonephritis • Acute glomerulonephritis - begins suddenly • Chronic glomerulonephritis -develops gradually over several years.
Kidney pain normally happens in the “flank” region, which is just below the bottom of rib cage.
Sign and symptoms • Cola-colored or diluted, iced-tea-colored urine from red blood cells in your urine (hematuria) • Foamy urine due to excess protein (proteinuria)
High blood pressure (hypertension) • Fluid retention (edema) with swelling evident in your face, hands, feet and abdomen • Fatigue from anemia or kidney failure. • Less frequent urination than usual.
Diagnosis • Urine analysis • Blood investigation • Culture • Renal biopsy
Management • Treatment depends on the cause of the disorder, and the type and severity of symptoms. • High blood pressure may be hard to control. Controlling high blood pressure is usually the most important part of treatment. • Dialysis and Transplant
Medications • Diuretics to reduce fluid retention • Medications to suppress the immune system Lifestyle Changes • Restrict salt and water intake. • Restrict intake of potassium, phosphorous, and magnesium. • Cut down on protein in the diet. • Maintain a healthy weight through diet and exercise. • Take calcium supplements.
Physiotherapytreatment • Patient education • Endurance Exercise • Walking test • walking, swimming, bicycling, aerobic dancing • Circulatory exercise
Precautions • Do not give an exercise to patient with consideration of these condition: • Changed their dialysis schedule • Changed their medicine schedule • Overeaten • Physical condition has changed; • Fever • Have joint or bone problems • Do not give exercises in an indoor, air-conditioned environment.
Discontinue routine earlier if experience any of the following: • shortness of breath • fatigue, • rapid or irregular heartbeat, • chest pain, • nausea, • leg cramps or dizziness.
NURSINGMANAGEMENT • History collection • Monitor fluid status • Prevention from infection • Prevent skin breakdown • Meet nutritional needs • Emotional support
NURSINGDIAGNOSIS • Fluid volume excess related to decreased urine output secondary to damaged nephrons • Activity intolerance related to fatigue • Imbalanced nutrition less than the body requirement related to anorexia • Fatigue related to increased metabolic demands and anemia • Risk for impaired skin integrity related to edema
COMPLICATION • Hypertensive encephalopathy • Acute cardiac decompensation • Acute renal failure
DEFINITION • It is a clinical state that includes massive proteinuria, hypoalbumineamia, hyperlipidemia and edema.
INCIDENCE • 2-6yrs of age • More in males
TYPES/CAUSES • Primary nephrotic syndrome • Primary disease known as idiopathic nephrosis, childhood nephrosis, or minimal change nephrotic syndrome.(MCNS) • 80% of cases with MCNS • Non specific illness (viral infection , URI) • Disease limited to kidney • Protenuria and edema
Secondary nephrotic syndrome: • Acute/chronic glomerular nephritis • Toxicity of drugs (trimethdione) • Rare • Sickle cell disease • Hepatitis • Malaria • TB, • Renal vein thrombosis • AIDS, • lymphoma, • infective endocarditis
Congenital nephrotic syndrome: • Hereditary • Recessive gene and autosomal disease. • Gene mutation
CLINICAL FEATURES • Edema around eyes, legs and labia • Anasarca (generalized body edema)
Ascites • Hydrothorax and hydrocele • Decrease urine output, urine appears to be frothy • Hematuria • Fever, rashes and joint pain • Pallor, Irritability • Loss of appetite but weight gain • Susceptibility of infection
DIAGNOSTICEVALUATION • 24Hrs urine total protein • Blood investigation: elevated cholestrol, albumin, urea
Therapeutic management • General measures • Prednisolone is the drug of choice 2mg/Kg/day orally in divided doses for 6 weeks Then 1.5mg/Kg single dose on alternate days for 6 weeks • Diuretic and salt poor albumin indicated –severe edema • Well balanced diet rich in proteins • Sodium, water restriction
NURSINGMANAGEMENT • Monitoring intake output • Urine examination • Daily weight measurement • Measurement of abdominal girth • Assessment of edema • Monitoring the vitals signs • Protect children from contact with infected roommates • Recreational therapy • Parental education • Serve alternative meals
NURSING DIAGNOSIS • Excess fluid volume related to retention of urine • Imbalanced nutrition less than the body requirement related to anorexia • Fatigue related to loss of protein • Disturbed body image related to edema • Activity intolerance related to fatigue • Risk for impaired skin integrity related to edema
COMPLICATIONS • Acute renal failure • Chronic kidney disease • Fluid overload • Infection • Pulmonary edema • Congestive cardiac failure • Growth retadation
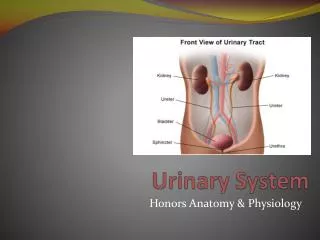
Urinary Tract Infection (UTI) Concept of “asymptomatic bacteria” in urinary tract
Causes • E. coli most common pathogen • Streptococci • Staphylococcus saprophyticus • Occasionally fungal and parasitic pathogens
Classificationof UTI • Upper tract: involves renal parenchyma, pelvis, and ureters • Typically causes fever, chills, flank pain • Lower tract: involves lower urinary tract • Usually no systemic manifestations
Classification of UTI Lower tract • Cystitis • Urethritis Upper tract • Pyelonephritis • Glomerulonephritis
Classification of UTI • Uncomplicated infection • Complicated infections • Stones • Obstruction • Catheters • Diabetes or neurologic disease • Recurrent infections
Types of UTIs • Recurrent—repeated episodes • Persistent—bacteriuria despite antibiotics • Febrile—typically indicates pyelonephritis • Urosepsis—bacterial illness; urinary pathogens in blood
Etiology and Pathophysiologyof UTI • Physiologic and mechanical defense mechanisms maintain sterility • Emptying bladder • Normal antibacterial properties and urine and tract • Ureterovesical junction competence • Peristaltic activity
Alteration of defense mechanisms increases risk of UTI • Organisms usually introduced via ascending route from urethra • Less common routes • Bloodstream • Lymphatic system
Contributing factor: urologic instrumentation • Allows bacteria present in opening of urethra to enter urethra or bladder • Sexual intercourse promotes “milking” of bacteria from perineum and vagina • May cause minor urethral trauma
UTIs rarely result from hematogenous route • For kidney infection to occur from hematogenous transmission, must have prior injury to urinary tract • Obstruction of ureter • Damage from stones • Renal scars
UTI is a common nosocomial infection • Often E. coli • Seldom Pseudomonas • Urologic instrumentation common predisposing factor
Clinical Manifestations of UTI • Symptoms • Dysuria • Frequent urination (>q2h) • Urgency • Suprapubic discomfort or pressure
Urine may contain visible blood or sediment (cloudy appearance) • Flank pain, chills, and fever indicate infection of upper tract (pyelonephritis)
Pediatric Manifestations • Frequency • Fever in some cases • Odiferous urine • Blood or blood-tinged urine • Sometimes NO symptoms except generalized sepsis