Download
1 / 37
370 likes | 391 Views
Explore the intricate factors influencing implantation failure in assisted reproduction, from endometrial receptivity to hormonal stimuli and genetic regulation. Discover the significance of cellular interactions and molecular pathways affecting successful implantation.

E N D
Habitual implantation failure /RM,RIF/ S. Škrablin
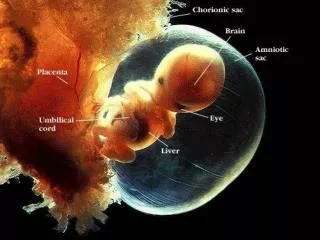
Successful implantation Materno-fetal dialogue Competent blastocyst receptive endometrium
“Window of implantation” Th1 phenomenon • 19-23 cycle day (6. day after ovulation!!!) • Stromal cells transformation into decidual cells: secretory granules, pinopodes, disappearance of mycrovilli…… • Cytokines, chemokines, ligands……. • dNK, macrophages, uDCs Regulatory role in trophoblast invasion APC “antigen presenting cells” Angiogenesis, decidualisation
LIF and p53 (Stewart LC, Nature 2007; 450:619, Hu W et al. Nature 2007; 450:721) HCG LIF Acquisition of adhaesion ligands and loss of inhibitory molecules LIF – receptor interraction endometrial receptivity
HOX gens Segmental body identity • HOX gens – endometrial development - steroid hormones function - elevated expression during secretory phase - with successful implantation increased decidual expression - regulation of morphological parameters of implantation window: pinopodes, beta 3 integrin, IGFBP1 - essential for implantation – low HOX genes expression during the secretory phase - infertility/Taylor et al.1999, Rackow and Taylor 2010/ “unexplained infertility” /Brosens et al., 2009/
HOX expression manipulation- increased implantation with EAI /in vitro //Bagot et al., 2000/
Leiomyoma deformity occlusion Low HOXA10 and BTEB1 exp. ■PCOS Decreased αvβ3 integrin, HOXA-10 and IGFBP-1 “Overexpression” of androgene receptors Absence of estrogen receptor-α downregulation during implantation window Overexpression ofsteroidreceptor coactivators - AIB1 and TIF2 Endometrial polyp Gamete transport Decreased IGFBP-1 i osteopontin Low progesteron receptors Implantation failure/Cakmak H, Taylor HS. 2011/
Endometriosis: - Decreased αvβ3 integrins and LIF - Low IL-11 and IL-11R - Absence of HOXA10 and HOXA11 increase - Elevated EMX2 - Progesteron resistence - Disregulation of PR-A / PR-B - HOX 10 promotor hypermetilation Hydrosalpinx Toxic effect of tubal secretions Decrease of avβ3 integrin and LIF-a Low HOXA10 expression ■Septum, arcuatus ■Sy Asherman ■ Thin endometrium ■ Ovarian stimulation ■ Adiposity ■ Trombophilia Impaired endometrial function Immunologic factors Implantation failure/Cakmak H, Taylor HS. 2011/
Hoxa 9-tubes Hoxa 11-cervix Hoxa 13-vagina Hox10/HOX10 geni –ECTOPIC AND EUTOPIC ENDOMETRIUM/Zanatta et. al., 2010/ “Mulleriosis” 11% female fetuses !!!!!! • Embrional remnants – regrowth during and after puberty • “De novo” creation of eutopic or ectopic endometrium – when, why, what is the initial stimulus ???? HOX10-epithelial, stromal and myometrial embriogenesis Expression is regulated by cyclical E/P variation Endometrial receptivity and nidation window
EAI/Zanatta et. Al., 2010/ In 50% no alfa 5 beta 3 integrin - Infertile with mild endometriosis /M. Donaghay, B.A. Lessey 2007/ Low FC, abnormal follicular maturation, Low oocyte quality /Toya et al. 2000/ - Poor oocyte quality - Implantation failure • Low endometrial alfa, beta integrin • No IL -11 i IL 11R i LIF-a • After GNRH analogues or ablation • increased HOX expression and • integrins • /Lessey i Young 1997, Daftary et al., 2007/ Ectopic towards eutopic endometrium - communication: ? Could radical surgery of ectopic endometrium assure normal eutopic edometrium function
Molecular differences Ectopic: 17beta-hydroxsteroid d., aromatase, P rec., ERbeta 140x P rezistence apoA-I – plasma, endometrium, HCG resistant /beta HCG can not inhibit apo A-I/Brosens et al., 2009/ “hallmark” of e. Medical od radical surgical silencing of extrauterine genes could PREVENT e. Radical surgery of e.foci DOUBLED success in ART cycles/Bianchi et al., 2009/
Hydrosalpinx: ►Flushing effect, pinopod malfunction, malfunction of endometrial epitelial cells…. ►Embriotoxic /animal studies/ ►Out of phase endometrium low integrins , LIF, HOX… Chl. inf. , PID: endometritis HSP- scar tissue - anti Chl HSP IgA – marker for unsuccessful IVF - HSP 10– tubal infertility - HSP 60- early misccariage PID , hydrosalpinx /Chukwuemeka et al, 2002/ IVF success after salpingectomy / Strandel et al., 2001, Cochrane dtb2002 /
Compared to infertile SM – decreased fertility /RR PR 0,30/ • /Somigliana et al. 2011/ IVF/ICSI – meta analysis/Bajekal , Li 2000/ Similar results 3 META ANALYSES: Pritts et al, 2009 Sunkara et al, 2010 Metwally et al, 2011. P <0,05
The effect of submucous fibroids/Rackow and Taylor, 2010/ • Decreased HOXA10, HOXA11, LIF, BTEB1 • MRNA HOXA 10 i HOXA 11 compared to intramural • Global – entire endometrium, not only beneath myoma • Size of myoma not important!!!!! Glycodelin, IL-10 – only with SM /Ben-Nagi J et al., 2010/
Inflammatory reaction with fibroids/Miura S et al., 2006/ • Monocyte chemotactic protein – (MCP-1), macrophage infiltration, PGF2alfa - SM and IM sigg. elevated compared to SSM, healthy myometrium or endometrium • Size of myoma not important!!!!!
The outcome of pregnancy with fibroidsUniv. Med. School Zagreb 2008-2012, N=135mean age 35,4 y. Skrablin et al. Eur J Obstet Gynecol Reprod Biol. 2005;118(1):115-6. • 17 previous myomectomy:17,6% • 35 previous delivery: 25, 9% • 84 first pregnancy: 62, 2% • 22 previous misccariage: 16, 2% • IVF: 9 (6,6%) Ap.1.:9,1 Ap.2.:9,4 *pH 7,26 Vaginal delivery: 39 (28, 8%) Complications: 6 (4, 4%) Ruptura uteri completa 1 Hysterectomia abd.: 5 N newborns >22 tj = 134 (1 triplets , 1 twins) Perinatal mortality 1/134 = 7,4%o 23 weeks, Apgar 1/0
Skrablin et al.. Successful pregnancy after spontaneous rupture of scarred uterus following fundal myomectomy. Eur J Obstet Gynecol Reprod Biol. 2005;121(2):251-2 The ooutcome of pregnancy after myomectomy Univ. Med. school Zagreb 2008-2012, N=50mean age 35,9 y. N = 52 newborns (3 twins) Perinatal mortality: 3/52= 57,6%o (26 gemin 31 ruptura 32 IUGR) • 15 previous birth: 30,0% • 27 first pregnancy: 54,0% • 9 previous miscarriage: 18,0% • 3 IVF: 6% Technique: 18 lap: 36,0 % 26 LPSC: 52,0% 2 Hys: 4% 1 sc: 2% 1 conversion lpsc to lap : 2% 2? Ap.1.:8,7 Ap.2:9,1 *pH: 7,16 Vaginal birth: 4 % Complications: 1 (2, 0%) Ruptura uteri completa 1 (31 tj., mors fetus in grav)
The effect of myomectomy SM • PCT – spontaneous pregnancies - 15% increase in fertility, outcome of pregnancy unknown /Casini ML et al., 2006/ - 10 reports – risk of complications after myomectomy can not be determined with certainty /Viswanathan et al., 2007/
The effect of myomectomy randomized “matched control”study/Shokeir T, et al. 2010/ SM Hys miomectomy N = 101 Hys – biopsy N=103 63,4% 28,2% pregnancy Success with op. with type O and I, but NOT with myoma type II
The effect of myomectomy /Pritts EA, Parker WH, Olive DL, 2009/ • IM N RR p (studies) CPR 2 3,76 n.s. LBR 1 1,67 n.s. SA 1 0,76 n.s. IM “..as yet no data to support myomectomy in the treatment of IM myomas to improve fertility outcome”
Tulandi, Barbieri, Falk, Uptodate 2011 • Asymptomatic leiomyomas - Suggestion not to postpone pregnancy, since leiomyomas, combined with advanced maternal age, may impair fertility and adversely impact pregnancy (Grade 2C) - Suggestion not to perform prophylactic myomectomy to prevent pregnancy complications (Grade 2C) • Infertile or a history of recurrent pregnancy loss: - Submucosal or an intracavitary component - myomectomy (Grade 2C). - Subserosal - against myomectomy (Grade 2C). - Intramural fibroids that do not distort the uterine cavity, other sources of infertility should be addressed. The decision to perform a myomectomy should be made based on patient preference and clinical factors (eg, obstructing of a fallopian tube or the cervical canal or failure of other infertility treatments). • IVF • Submucosal fibroid or an intramural fibroid that deforms the uterine cavity should be removed (Grade 2C).
Implantation with endometrial polyp • Low IGFBP1 and osteopontin • Low P receptor expression – P resistency • After polypectomy elevation of IGFBP1, osteopontin levels /Ben-Nagy et al., 2009/
The effect of polypectomy in subfertile women S - IVF/ICSI/IUI Polipectomy C -IVF/ICSI/IUI –Without polipectomy • Polyps • - prior to IVF • should be removed • during the course of COH- • management individualized • /Afifi K, et al., 2010/ The only randomized Perez-Medina et al.2005 IUI randomizirana Lass et al.1999 Isikoglu et al.2006
Septum uteri/Revel, 2012/ • Blood flow dearranged • UTERUS ARCUATUS - less than 1 cm, - probably without ill effect • Hys - simple • Still dubious whether to perform op. before conception • Peer opinion poll –in support of prophylactic operation less than 50% of experts!!!!/M.J. Cohen, T.S. Rosenzweig, A. Revel, 2007/
Asherman Sy • Sperm transport or implantation compromised • Infertility in 802 / 2151 (43%)-depending on severity PR – no operation 51% (540 of 1052), - no therapy 46% (133 of 292) - Hys 74% (468 of 632) /J.G. Schenker, E.J. Margalioth 1982/ • After surgery : IUD ili baloons • Bone marrow stem cells - regeneration/H.S. Taylor 2004/
Thin endometrium • Problem : elevated oxygen in endometrium/R.F. Casper 2011/ • But, implantation could be successful even with very thin endometrium/3.7 mm/J.H. Check, R. Cohen 2011/ • 3D – endometrial volum compared to 2D endometrial thickness - not better for IVF success estimation /J. Alcazar 2006/
Ovarian stimulation • E elevation – endometrial receptivivity decreased • CPR per transfer – sigg. better after transfer of frozen embria /B.S. Shapiro et al., 2011/
PCOS • Oligoovulation • P low and its regulatory function dearranged, constant unopposed E2 • Low alfa and beta integrin, HOX-10 i IGFBP1 during secretory phase even in those with ovulations • Elevated androgens - decreased HOX 10 expression • Elevated A receptors, no downregulatiom Ealfa receptors Low receptivity and steroid receptor disregulation The consequence of low P or insulin/androgen imbalance? /Cakmak H, Taylor HS, 2011/
Clinical US– thicknes and texture - 6mm No correlation with hystology “Proliferative phase defect” – Subendometrial blood flow – no correlation with implantation success or failure ■ SHG In general: capability of US methods to estimate implantation is low/Cakmak H i Taylor Hs, 2011/ ■ Hys PHD Endometrial dating – no criteria for window of implantation Difficult and unpredictable in stimulated cycles Cannot differentiate fertile from infertile population /Coutifaris i sur. 2004/ ■ Markers: - p53/Goodman et al., 2009/ - gene profiling /microarray/ or proteomic analysis- apoA-I /Brosens et al., 2011/ - alfa, beta integrin, mucin, LIF,HOXA10, “endometrial function test-EFT” …..still experimental /Dubowy i sur. 2003/ - trombophilia ENDOMETRAL EVALUATION MRI-junctional zone
LIF and IL 11 Uterine flushings – - LIF levels - estimation of successful implantation in IVF/Makkar et al., 2006/ - low levels in infertile women/Delage et al., 1995/ - LH +2 can predict IVF success in the next cycle/Mikolajzyk et al. 2007/ FUTURE – estrimation of endometrial function before aspiration IL 11mRNA - low levels in trophoblast and plasma in anembrionic gestation or miscarriage/Koumantaki et al., 2001/ Therapy???/Brinsden et al 2009/
Endometriosis Fibroid Polyp Hydrosalpinx PCOS Adenomyosis Endometritis Trombophilia - Ablation, GNRH agonists - Miomectomy - Polypectomy - Salpingectomy or tubal occlusion - Weight loss, metformin - GNRH agonists, surgery -Antibiotics - LMWH Treatment - today Heparin, aspirin – vaskularization Cortikosteroids – immunological tolerance LIF, progesteron – receptivity IG – immunologic tolerance
Treatment– tomorrow…. • Reproductive surgery • Endometrial scratching/Barash A et al., 2003/ • “Priming” - locally instilationor parenteral: granulocyte colony-stimulating factor, HCG or piroxicam/N. Gleicher et al., 2011, R. Mansour et al., 2011, H.S. Moon et al., 2004/ • Stem cells /Taylor HS, 2004, Du H, Taylor HS,2010/ • Heparin, metformin – stimulation of gene expression in endometrium/Germeyer et al., 2011/ • Embryo culture with adhaesion promoting factors( hyaluronic acid, heparanase, VEGF)/ Revel et al., 2005, Hannan NJ et al., 2011/ • PIF /Duzy K., et al., 2011/ …………………………….. “Leukonorm” “Lenograstim” ……. Gene “improvement” Immunomodulation