Download
1 / 43
430 likes | 565 Views
MBQIP Phase 2 Focus on HCAHPS. Critical Access Hospital Presentation July 23 2014. Objectives. Define the 3 phases of the Office of Rural Health MBQIP program Describe Hospital Consumer Assessment of Health Providers and Systems ( HCAHPS)

E N D
MBQIP Phase 2Focus on HCAHPS Critical Access Hospital Presentation July 23 2014
Objectives • Define the 3 phases of the Office of Rural Health MBQIP program • Describe Hospital Consumer Assessment of Health Providers and Systems (HCAHPS) • Understand the value of engaging in the HCAHPS process • Identify the benefits and challenges of HCAHPS • Review HCAHPS Vendor Directory
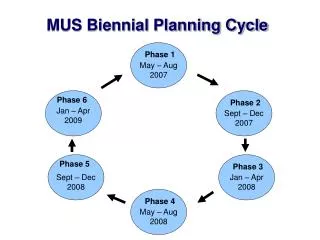
Medicare Beneficiary Quality Improvement Project • Began September 2011, voluntary-register on Quality Net 100% participation goal by FY 2014 • Nationwide quality improvement plan for rural healthcare • Improves access for Medicare beneficiaries served, including EMS • Voluntary CAH quality benchmarking & reporting to CMS Hospital Compare • Builds a national data base to demonstrate effect of rural quality improvement initiatives • Phase I Process measures for inpatient Pneumonia & HF • Phase II- Outpatient measures 1-7 and HCAHPS • Phase III-Pharmacy CPOE review of orders in 24 hours & ED transfer communication & report quality improvement data to state
MBQIP – Why participate? • Promotes accountability & public disclosure • Future of all hospital reimbursement will soon be tied to performance-Get ahead of the curve • Only statistically significant volumes will be reported (>25 cases) • Gives benchmark data to analyze and guide performance improvement • It’s the RIGHT thing to do ! Evidence drives improvement
The Patient Experience of Care is Fundamental to Clinical Improvement • Understanding the patient experience of care is not an add-on activity: it should be used as a fundamental element in your other improvement efforts. • For those working on the GHA Partnership for Patients Hospital Engagement Network (HEN) your work will benefit directly from your efforts to improve the patient experience of care. • Patient-centered care is a driver of clinical outcomes • Employee and patient engagement are 2 sides of one coin • HCAHPS assesses key factors in ADEs and readmissions
New Care Transition composite will be publicly reported on Hospital Compare, October 2014
Approved Vendor list • Review attachment A2
HCAHPS reports • Hospital level results reported at http://www.hospitalcompare.hhs.gov • Additional reports on HCAHPS website (http://hcahpsonline.org) • Top box scores by state • Percentiles • Correlations • Hospital Characteristics
Communication with Nurses During this hospital stay… • how often did nurses treat you with courtesy and respect? (Q1) • how often did nurses listen carefully to you? (Q2) • how often did nurses explain things in a way you could understand? (Q3)
Communication with Nurses Success Strategies: • Hourly Rounding • White Boards/Care Boards • Bedside Reporting • AIDET • Ascertain need for and obtain language assistance.
Communication with Doctors During this hospital stay… • how often did doctors treat you with courtesy and respect? (Q5) • how often did doctors listen carefully to you? (Q6) • how often did doctors explain things in a way you could understand? (Q7)
Communication with Doctors Success Strategies: Using strategic language • I am washing my hands for your SAFETY.” • “I have TIME to answer your questions.” • “I want you to be INVOLVED in your treatment plan” • “I want to be sure I EXPLAIN everything to you…” • “To protect your PRIVACY, let me close the curtain.” • “For your COMFORT, I ordered pain medicine...” • “I want to keep you INFORMED…” • “I want to make sure we are THOROUGH” • “You are in good hands with the nurses on this floor.” • STUDER
Responsiveness of Hospital Staff During this hospital stay…. • after you pressed the call button, how often did you get help as soon as you wanted it? (Q4) • How often did you get help in getting to the bathroom or in using a bedpan as soon as you wanted? (Q11)
Responsiveness of Hospital Staff • Success Strategies: • “No Pass” Zones • Hourly rounding
Pain Management During this hospital stay, • how often was your pain well controlled? (Q13) • how often did the hospital staff do everything they could to help you with your pain? (Q14)
Pain Management Success Strategies: • Patients’ experience of pain management is not entirely dependent on their level of pain • Pain management perceptions are affected by many factors, including: • Effective communication with physicians and nurses • Responsiveness • Empathy • Set Reasonable Expectations • Be candid about the pain to be expected • Keep the patient informed • e.g., use the white board to keep the pain goal and plan visible, as well as next scheduled medication • Respect the Patient’s Expertise • Discuss options, tradeoffs, and preferences, including what has worked previously • Develop pain goals and a plan • Explain the purpose of the pain scale • Ask patients contextual questions • e.g., at what point on the scale would they take an over the counter medicine for pain
Communication of Medications Before giving you any new medicine, • how often did hospital staff tell you what the medicine was for? (Q16) • how often did hospital staff describe possible side effects in a way you could understand? (Q17)
Communication of Medications Success Strategies: • TV Education channel • Involving multidisciplinary approach • Dietician • Respiratory • Clinical Pharmacist • White Boards • List new Medications • Document teaching for cross communication and reinforcement
Discharge Information During this hospital stay • did doctors, nurses or other hospital staff talk with you about whether you would have the help you needed when you left the hospital? (Q19) • did you get information in writing about what symptoms or health problems to look out for after you left the hospital? (Q20)
Discharge Information Success Strategies: • Identify the correct medicines and a plan for the patient to obtain and take them. • Use “target tool” to educate the patient about his or her diagnosis and self management
Care Transition • During this hospital stay, staff took my preferences and those of my family or caregiver into account in deciding what my health care needs would be when I left.(Q23) • When I left the hospital, I had a good understanding of the things I was responsible for in managing my health. (Q24) • When I left the hospital, I clearly understood the purpose for taking each of my medications. (Q25)
Care Transition Success Strategies: • Make appointments for follow-up medical appointments and post discharge tests/labs. • Organize post-discharge outpatient services and medical equipment. • Provide telephone reinforcement of the Discharge Plan.
HCAHPS: Global Items Overall rating of the hospital • Using any number from 0 to 10, where 0 is the worst hospital possible and 10 is the best hospital possible, what number would you use to rate this hospital during your stay? (Q21) Recommendation of hospital • Would you recommend this hospital to your friends and family? (Q22)
Individual Items • Cleanliness of Hospital Environment (Q8) • Quietness of Hospital Environment (Q9)
Individual Items Success Strategies: • Staff returns if patient is not in room during cleaning • Gold stickers on toilet paper • From: leaving tent cards To: “Get Well” cards • Revise job descriptions and related materials • e.g., role is to prevent nosocomial infections • Bring out Quiet signs • Inquire regarding quietness on unit during rounding • Ask about and preserve patient sleep rituals • e.g., a cup of tea, reading material, snack • Change EKG batteries & leads at a.m. shift change
How will HCAHPS Reinforce Focus on Quality? • Patient-Centered care is a quality indicator • Quality no longer the domain of just the clinicians • Gives a voice to the patient perception of safety • Highlights communication issues/barriers • Patient-centered care actively involves patients in their care • More senior leaders are engaged and interested in delivering patient-centered care
The Patient Experience of Care is Fundamental to Clinical Improvement • HCAHPS is viewed as a valuable tool to help organizations achieve multiple objectives • HCAHPS is part of a coordinated, comprehensive approach to partnering with patients and families • Everyone works together as a team to identify opportunities for improvement, innovate and implement strategies, and celebrate success
HCAHPS Challenges • Cost • Obtaining a meaningful response • Public perception that low volume could be a negative trait for a care provider
HCAHPS Success Depends on A Strong Foundation Foundational Elements of Patient-Centered Care • Leadership • Patient/Family Partnership • Workforce Engagement • Data Use/Performance Improvement
Mine the Data for Solutions, Not Just Problems • View patient experience data as an opportunity for “appreciative inquiry” • Reveal hidden innovation within your own organization • Examine improvement (including change in “bottom box” scores), not just achievement • Put HCAHPS data in context with other qualitative and quantitative information about the patient and staff experience • Preserve relationships by noting what is working well
Other Important Sources of Information Patient Experience Staff Experience Employee Engagement Data Staffing Levels Patient Safety Culture Survey Data • Post-discharge phone calls • Rounding • Patient and family focus groups • Patient and family advisory council/advisors • Ombudsman/patient advocate programs • Compliments
Shadowing • A unique opportunity to gain a perspective on the experience through the patient’s eyes • Request patient permission • Explain role is to observe and identify opportunities to improve care that will help others • Record observations • Patient/family perspective • Your own reactions http://www.pfcc.org/go-shadow/
Additional Resources AHRQ/HRET Patient Safety Learning Network (PSLN) HCAHPS National Teleconference Series http://www.psl-network.org/ Fundamentals of HCAHPS Using HCAHPS Data Effectively Nurse Communication Responsiveness Medication Communication Discharge Information Physician Communication and Engagement Pain Management Clean & Quiet
Questions? It is not just about scores, financial indicators, public reporting, % of always…it is about compassionate care and saving lives
GHA Contact Information Kathy McGowan, Vice President of Quality & Safety kmcgowen@gha.org 770-249-4519 Joyce Reid, Vice President of Community Health Connections jreid@gha.org 770-249-4545 Lisa Carhuff, Quality Improvement/Patient Safety Specialist Rural and Critical Access Hospitals lcarhuff@gha.org 770-249-4553