Download

1 / 16
160 likes | 183 Views
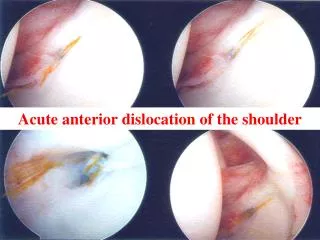
Necessity of Radiographs in Anterior Shoulder Dislocation. Evidence in the ED Matt Fields June 27, 2007. Studies. G. Hendey and K. Kinlaw, Clinically significant postreduction radiographic abnormalities in anterior shoulder dislocations, Ann Emerg Med 28 (1996), pp. 399–402.

E N D
Necessity of Radiographs in Anterior Shoulder Dislocation Evidence in the ED Matt Fields June 27, 2007
Studies • G. Hendey and K. Kinlaw, Clinically significant postreduction radiographic abnormalities in anterior shoulder dislocations, Ann Emerg Med28 (1996), pp. 399–402. • M. Shuster, R. Abu-Laban and J. Boyd, Prereduction radiographs in clinically evident anterior shoulder dislocation, Am J Emerg Med17 (1999), pp. 653–658. • M. Emond, N. Le Sage, A. Lavoie and L. Rochette, Clinical factors predicting fractures associated with anterior shoulder dislocation, Acad Emerg Med11 (2004), pp. 853–858. • G. Hendey, M. Chally, and V. Stewart, Selective Radiography in 100 patients with suspected shoulder dislocation, J Emerg Med 31 (2006), pp. 23-28
Hendey and Kinlaw. 1996 • Retrospective chart review • Evaluating utility of post reduction x-rays • 175 Anterior Shoulder Dislocations • All got pre and post reduction x-rays • 3 avulsion fractures identified on post-reduction x-ray (not on pre) • 14 new Hill-Sachs Deformities • Only one case of persistent dislocation that was subsequently reduced. This was the only case that changed management. Ann Emerg Med 28 (1996), pp. 399–402
Hendey and Kinlaw. 1996 • Conclusion • Postreduction radiographs rarely reveal any clinically significant abnormality after an anterior shoulder dislocation has been reduced. Ann Emerg Med 28 (1996), pp. 399–402
Shuster et al. 1999 • Prospective, evaluating utility of pre-reduction x-rays • 97 patients presenting to 2 ski-hill clinics and a rural ED (Banff, Colorado) with possible dislocation as assessed by triage staff. • At the rural ED, physician certain of dislocation in 40/59 cases on history and physical. All 40 confirmed to have dislocation by x-ray. • 36 cases at ski-hill clinic all reduced without x-ray. • Prereduction radiograph (when performed) did not change management and added 29.6 +/- 12.68 minutes to treatment. Am J Emerg Med 17 (1999), pp. 653–658.
Shuster et al. 1999 • Conclusion • Experienced physicians are accurate at diagnosing anterior shoulder dislocation from history and physical. • Prereduction x-rays do not alter management and delay treatment. Am J Emerg Med 17 (1999), pp. 653–658.
Shuster et al. 1999 • This paper also notes that post-reduction films did not change acute management. However the authors believe that post-reduction x-rays are good because they reveal fractures, and thus to identify the need for additional treatment or changes to the rehabilitation program. Am J Emerg Med 17 (1999), pp. 653–658.
Emond et al. 2004 • Retrospective Study over 5 years period to compare profiles of those having a clinically important fracture with their shoulder dislocation and those sustaining a non-complicated shoulder dislocation. • 334 patients included: 85 (25.5%) had a clinically important fracture-dislocation, 249 (74.5%) had a non-complicated dislocation. Acad Emerg Med 11 (2004), pp. 853–858.
TABLE 2. Presence of Clinically Important Fracture-dislocation by Clinical Factors Predictor Clinically Important Fractures (n = 85) (25.5%) Noncomplicated Dislocations (n = 249) (74.5%) Crude Odds Ratio (95% CI) Adjusted Odds Ratio (95% CI) Atraumatic 0 47 (100%) —* — Presence of Clinically Important Fracture-dislocation by Clinical Factor
Emond et al. 2004 • Odds Ratio of Each Factor for having a fx • Age > 40 years: 5.18 (95% CI = 2.74 – 9.78) • First Episode: 4.23 (95% CI = 1.82 – 9.87) • Mechanism: 4.06 (95% CI = 1.95 – 8.48) • Predictive Model using any 1 of 3 risk factors: • 97.7% Sensitivity (95% CI = 91.8% - 99.4%) • 22.9% Specificty (95% CI = 18.1% - 28.5%) • 96.6% NPV (95% CI = 88.3% - 99.6%) Acad Emerg Med 11 (2004), pp. 853–858.
Hendey et al. 2006 • Prospective study to validate algorithm based on findings from previous studies. • Physicians were given algorithm for ordering pre and post reduction films, but were allowed to deviate from guidelines by clinical judgment. J Emerg Med 31 (2006), pp. 23-28
Hendey et al. 2006 • Performed phone contact at 1 and 30 days and chart review at 30 days. • Able to contact 76% at day 1 and 61% at both days. 18 of 25 patients who received no radiographs were reached with no missed fractures. 75 of 76 patients reached satisfied with ED care. • 40% of all patients followed up in ortho clinic. • 11/30 who had pre and post films. 3 had repeat films. • 27/64 who had one or no film. 9 got shoulder films in clinic. • No missed fractures or persistent dislocations. J Emerg Med 31 (2006), pp. 23-28
HUPism • In patients under 40 with non-traumatic recurrent anterior shoulder dislocation x-rays are not necessary. • In all other cases a pre-reduction x-ray should be obtained, but if no clinically significant fracture is seen then a post-reduction x-ray is not necessary.