Download
1 / 1
10 likes | 124 Views
Brown- Sequard : A Rare Stroke Mimicker Jamie Knecht DO, Domenico Mastandrea DO, Ulrich Reischel MD. Introduction. Clinical Course.

E N D
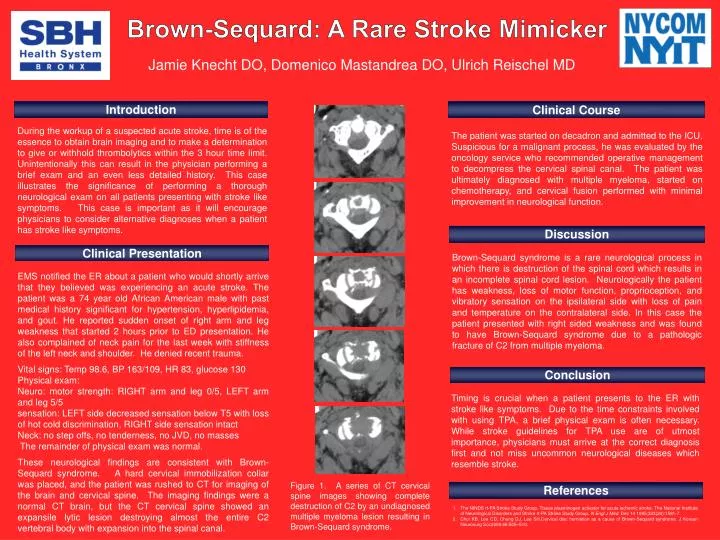
Brown-Sequard: A Rare Stroke Mimicker Jamie Knecht DO, DomenicoMastandrea DO, Ulrich Reischel MD Introduction Clinical Course During the workup of a suspected acute stroke, time is of the essence to obtain brain imaging and to make a determination to give or withhold thrombolytics within the 3 hour time limit. Unintentionally this can result in the physician performing a brief exam and an even less detailed history. This case illustrates the significance of performing a thorough neurological exam on all patients presenting with stroke like symptoms. This case is important as it will encourage physicians to consider alternative diagnoses when a patient has stroke like symptoms. The patient was started on decadron and admitted to the ICU. Suspicious for a malignant process, he was evaluated by the oncology service who recommended operative management to decompress the cervical spinal canal. The patient was ultimately diagnosed with multiple myeloma, started on chemotherapy, and cervical fusion performed with minimal improvement in neurological function. Discussion Clinical Presentation Brown-Sequard syndrome is a rare neurological process in which there is destruction of the spinal cord which results in an incomplete spinal cord lesion. Neurologically the patient has weakness, loss of motor function, proprioception, and vibratory sensation on the ipsilateral side with loss of pain and temperature on the contralateral side. In this case the patient presented with right sided weakness and was found to have Brown-Sequard syndrome due to a pathologic fracture of C2 from multiple myeloma. EMS notified the ER about a patient who would shortly arrive that they believed was experiencing an acute stroke. The patient was a 74 year old African American male with past medical history significant for hypertension, hyperlipidemia, and gout. He reported sudden onset of right arm and leg weakness that started 2 hours prior to ED presentation. He also complained of neck pain for the last week with stiffness of the left neck and shoulder. He denied recent trauma. Vital signs: Temp 98.6, BP 163/109, HR 83, glucose 130 Physical exam: Neuro: motor strength: RIGHT arm and leg 0/5, LEFT arm and leg 5/5 sensation: LEFT side decreased sensation below T5 with loss of hot cold discrimination, RIGHT side sensation intact Neck: no step offs, no tenderness, no JVD, no masses The remainder of physical exam was normal. These neurological findings are consistent with Brown-Sequard syndrome. A hard cervical immobilization collar was placed, and the patient was rushed to CT for imaging of the brain and cervical spine. The imaging findings were a normal CT brain, but the CT cervical spine showed an expansilelytic lesion destroying almost the entire C2 vertebral body with expansion into the spinal canal. Conclusion Timing is crucial when a patient presents to the ER with stroke like symptoms. Due to the time constraints involved with using TPA, a brief physical exam is often necessary. While stroke guidelines for TPA use are of utmost importance, physicians must arrive at the correct diagnosis first and not miss uncommon neurological diseases which resemble stroke. Figure 1. A series of CT cervical spine images showing complete destruction of C2 by an undiagnosed multiple myeloma lesion resulting in Brown-Sequard syndrome. References • The NINDS rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. Dec 14 1995;333(24):1581-7. • Choi KB, Lee CD, Chung DJ, Lee SH.Cervical disc herniation as a cause of Brown-Sequard syndrome. J Korean Neurosurg Soc2009;46:505–510.