Download
1 / 95
970 likes | 1.01k Views
Explore chest injuries with Dr. Karen D'Sa, covering anatomy, mechanism of injury (blunt, penetrating), pathophysiology, assessment, investigations, and treatment modalities for potentially deadly conditions. Gain insights into managing common thoracic trauma cases effectively.

E N D
CHEST INJURIES DR. KAREN D’SA
Introduction • Anatomy • Mechanism of Injury: Blunt trauma • Penetrating injury • Classification • Pathophysiology • General Assessment :A,B,C • Investigation • Treatment : deadly dozen , detected later
Introduction • 70% of trauma deaths - thoracic injuries • 2/3rds are alive when they reach the ER • Mostly patient presents with blunt trauma to chest wall • Only 15% require surgery
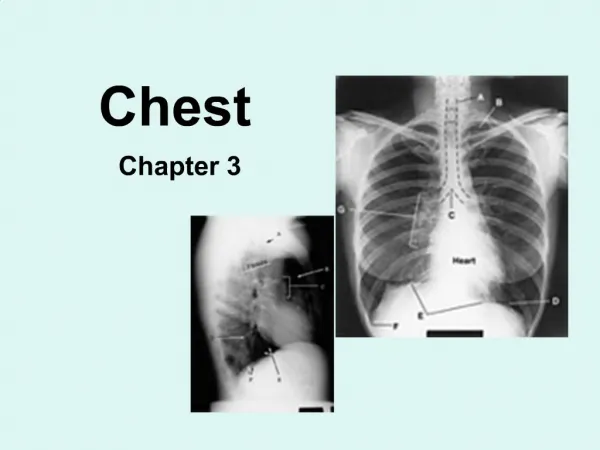
ANATOMY • 12 pairs of ribs • Pleural cavity - 3 litres each side • Contents : lungs, heart, aorta, SVC and IVC, trachea and major bronchi, esophagus • Intercostal neurovascular bundle - inferior border of rib
Mechanism of injury • Blunt – high velocity, low velocity, crush • Penetrating – a. sharp b. shotgun
High velocity impact injuries • Sudden deceleration • “Chest wall is intact” • “Bell Clanger effect” • Anterior chest wall contusion –myocardial injury
Low velocity impact injuries • “Direct damage to bony thorax” • No stress or compression forces to damage aorta or diaphragm
Penetrating chest wounds • Simple to deal with • “Sucking wound”
Pathophysiology “TISSUE HYPOXIA” • Hypercarbia and metabolic acidosis. • Causes of hypoxia: 1. Airway obstruction 2. Blood loss 3. Lung parenchymal injury 4. Tension pneumothorax 5. Severe myocardial injury
Assessment Symptoms: Shortness of breath Pain Respiratory distress Signs: • Tachypnoea Shock • Hemoptysis Cyanosis • Chest wall contusion Flail chest
Open wounds • Distended neck veins - SVC obstruction • Tracheal deviation • Emphysema • Bony crepitus • Breath sounds • Dullness, hyperresonance on percussion
Investigations • Usually AP, often supine, frequently in poor inspiration. • So, a challenge to interpret.
Deadly dozen 1.Airway obstruction 2. Tension Pneumothorax 3. Open Pneumothorax 4. Flail Chest 5. Massive Hemothorax 6. Cardiac Tamponade
Detected later 7. Aortic rupture 8. Pulmonary contusion 9. Tracheal / bronchial tree injury 10. Myocardial contusion 11. Diaphragmatic injuries 12. Esophageal injuries
1. Airway obstruction • Fracture/ post. dislocation at sternoclavicular joint • Rx : intubation, closed reduction
2. Tension Pneumothorax Each time we inhale, the lung collapses further. There is no place for the air to escape..
“One way valve” • Mechanism of injury : air enters but does not exit • Causes : • Intubated pts - positive pressure ventilation – most common cause. • Decreased lung compliance (difficulty in • squeezing the bag valve device) in the intubated patient
InvestiGATION • X-RAY FINDINGS • Collapse of lung • Shift of mediastinum • Depression of ipsilateral diaphragm
TREATMENT Insertion of chest tube connected to water seal drain
Chest tube • Chest tube – 5 th ICS anterior to midaxillary line at upper border 6th rib directed posteriorly and superiorly. • 2 cm transverse horizontal incision at top of 6th rib, puncture the pleura with tip of clamp and put a gloved finger into incision to avoid injury to other organs and to clear any adhesions/clots. • Clamp proximal end of tube and advance through desired length. Look for fogging with expiration or listen for air movement.
Indications for emergency room thoracotomy • Acute pericardial tamponade unresponsive to cardiac massage • Exsanguinating intra-thoracic haemorrhage • Intra-abdominal haemorrhage requiring aortic cross clamping • Need for internal cardiac massage
Indications for urgent thoracotomy • Chest drainage >1500 ml or >200 ml per hour • Large unevacuated clotted haemothorax • Developing cardiac tamponade • Chest wall defect • Massive air leak despite adequate drainage • Proven great vessel injury on angiography • Proven oesophageal injury • Proven diaphragmatic laceration • Traumatic septal or valvular injury of the heart
Open Pneumothorax Inhale
Open Pneumothorax Exhale
Open Pneumothorax Inhale
Open Pneumothorax Exhale
Open Pneumothoarx Inhale
Open Pnuemothorax Inhale
Mechanism of injury • Caused by penetrating injury • “Sucking chest wound” • Signs and symptoms are proportional to the size of defect; when defect > 2/3 diameter of trachea/glottis • Red Bubbles on Exhalation from wound
Investigations x-ray • Supine AP view has limited sensitivity: 50% • Visceral pleural line • Deep sulcus sign • Can see vessels • Subpulmonic air sign • Sharp heart border/hemidiaphragm sign • Increased lucency over lower chest
Management • Needle decompression– II ICS in MCL line – hissing sound of air exit confirms • Chest tube – into fifth ICS anterior to midaxillary line at upper border 6th rib directed posteriorly and superiorly.
Flutter Valve • Asherman Chest Seal
4. Flail Chest • The breaking of 2 or more ribs in 2 or more places
2 or > ribs segmental #. • Paradoxical respiration • Pendulum movement • Mediastinal flutter – shock • ABG shows respiratory failure with hypoxia
Management • Intubate (majority) • Pneumothorax is commonly associated and requires decompression. • Avoid volume overload with I.V fluids. • Use Gloved hand as splint till bulky dressing can be put on patient