Download
1 / 32
340 likes | 958 Views
Kienbock disease ( an overall View ). Mohamad Othman , MD 4-10 - 2012. Definition & history. - KD ( or lunatomalacia ) is an idioopathic AVN of carpal lunate which may lead to collapse of the bone and arthritis in the advanced stage.

E N D
Kienbock disease ( an overall View ) Mohamad Othman , MD 4-10- 2012
Definition & history - KD ( or lunatomalacia ) is an idioopathic AVN of carpal lunate which may lead to collapse of the bone and arthritis in the advanced stage - first described in 1843 by Peste in cadaver dissections. - Robert Kienbock ( 1910) , a radiologist, described the x-ray changes associated w KD.
Epidemiology • 15 and 40 years • dominant wrist of men engaged in manual labor Natural history of KD remains unclear & un-predictable
Aetiology : - unknown ; theories : Fault plate hypothesis: Intrinsic ( lunate) & extrinsic factors ----- elastic deformation of trabeculae 2ry to loading ----- fault plates ---- wall off & interfere w capillary bl. Flow ----- AVN - repetitive microtrauma in the lunate at risk ( predisposed lunate ) ;
Extrinsic factors: • capitate • - lunate loading • - ulnar variance : • ulnar-negative variant wrist is common association ( Hulten, 1928). • ulnar-positive variant • - load type • - instability
Intrinsic factors: - shape of lunate - trabecular pattern - cortical load - lunate vascular anatomy
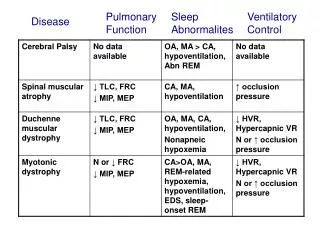
Staging ( Modified Lichtman Classification ) • Stage I: Radiographicallynormallunate or with small fracture lines • Stage II: Sclerosis of lunate • Stage III A: Collapse or fragmentation of lunate • Stage IIIB: Lunate collapse with carpal malalignmentie; proximal migration of capitate (carpal height ratio <0.54 ± 0.03) and fixed hyperflexed rotation of scaphoid( DISI)[radioscaphoid angle > 60] • Stage IV: Generalized wrist arthrosis
Stage-I Stage-II Stage-III Stage-IV
Clinical picture - Complaint may precede XR changes - Varies according to stage - Pain. Tenderness ,swelling, clunk w deviation, dec ROM , weak grip Investigations - Plain XR : views….. Measurements…. Staging. - CT - Scintigraphy - MRI : earliest diagnosis : uniform low signal in T1
Stahl index: Normally;B/A= 50% Carpal height ratio
Differential diagnosis: - ulnar impaction synd. ( MRI) - DRUJ arthritis - LunateFx , intraoss ganglion, enchondroma.
Treatment Objectives: (a) precollapse (b) postcollapse • Methods: • Established methods: • Direct vascularization • Indirect vascularization ( unloading procedures): • joint-levelling procedures • limited carpal fusions • Salvage procedures: • PRC • wrist arthrodesis • Optional & controversial methods: • - conservative • Lunateexcision ± replacement ( PL tendon ball , silicon, titanium) • - Core decompression of distal metaphysis of R & U • - Temporary ST pinning ; 3-6 mo . Stage III • - External fixation • - RSO in stage IIIB • - RO + VBG in stage III • - Wrist denervation; stage IV • - Arthroscopic debridement
Treatment Algorithm Stage I: Controversial ; not completely-unload lunate. Choice in transient ischemia. After 3 mo, aggressive management as stage II Stage I, II, or IIIA with Ulnar-Negative Variance : (1) Lunate unloading by joint-leveling procedures ( RS > UL) or (2) Lunate revascularization by VBG Stage I, II, or IIIA with Ulnar-Positive or Ulnar-Neutral Variance : (1) unloading by Capitate shortening ± capitate-hamate fusion or radius ost. (2) VBG ( ± STT-pinning)
Treatment Algorithm ( cont.) Stage IIIB : -intercarpal fusions (STT and SC ) - Proximal row carpectomy ( PRC) -RSO -Lunate excision Stage IV : - conservative - Proximal row carpectomy - wrist fusion-
Radial shortening osteotomy • Approach ; volar > dorsal • 2-3mm ( not > 4mm ; UC impaction ) • Meaphyseal / meta-diaphyseal • Not decrease ROM • Not in ulna positive wrist
Ulnar lengthening osteotomy Disadvantages;
Distal radius wedge osteotomy - Stage II or III w ulna-neutral or positive wrist - Lateral closing wedge osteotomy: decrease RU-inclination thus shifting press from lunate - Medial closing osteotomy or lat opening wedge o - Step- cut osteotomy
Capitate shortening osteotomy CSO + capito-hamate fusion
VBG • Sources: • - Base of 2nd or 3rd metacarpal • Neck of 2ndmeatacarpal • 1,2 ICSRA • - 2,3 ICSRA • - 4th or 5th CA • - Hori technique • - Pisiform • PQ • + unloading procedure: • - external fixator or • - temporary STT-pinning or • - radius osteotomy
2,3 ICSRA VBG 1,2 ICSRA VBG
4th CA VBG : retrograde flow through 5th CA from dorsal itercarpal arch
Limited carpal fusion • - Objective : redistribute stresses away from lunate • - Correct scaphoidmalrotation 1st • - SC / STT • Decreases ROM • Excise lunate; only if fragmented w marked synovitis
Temporary STT-pinning Triscaphe (STT) fusion SC- fusion
Prox raw carpectomy Total wrist fusion
Incisions for wrist denervation Core decompression of distal metaphysis of R & U
وشكرا THANK YOU والسلام عليكم ورحمة الله وبركاته