Download
1 / 31
350 likes | 958 Views
The Urinary System part 1. Ana H. Corona, DNP, FNP=BC July 2013. Kidney Size. ( determined by renal ultrasound) Average size: 10-12 cm Small kidneys vs. Enlarged kidneys ( Hydronephrosis ). Components of Nephron. Glomerulus Bowman’s capsule Proximal convoluted tubule

E N D
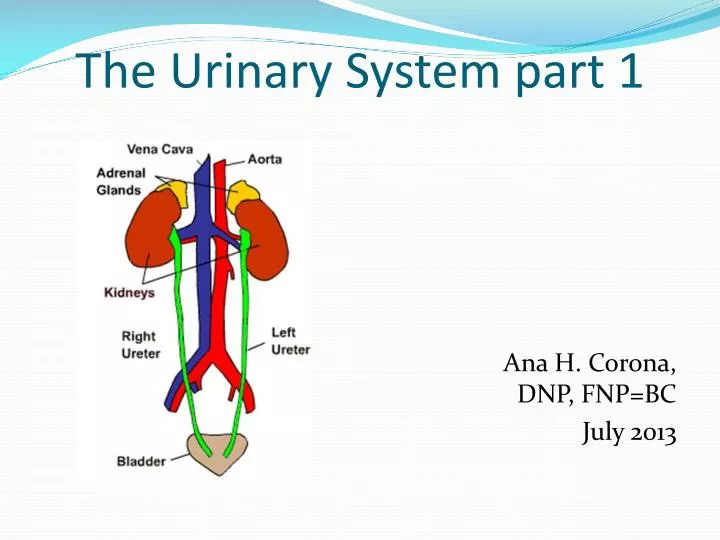
The Urinary System part 1 Ana H. Corona, DNP, FNP=BC July 2013
Kidney Size • (determined by renal ultrasound) • Average size: 10-12 cm • Small kidneys vs. Enlarged kidneys (Hydronephrosis)
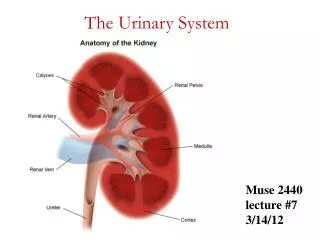
Components of Nephron • Glomerulus • Bowman’s capsule • Proximal convoluted tubule • Loop of Henle • Distal convoluted tubule • Collecting duct
Normal Renal Function • Depends upon the adequate and interrelated functioning of the CV system, nervous system, endocrine system, and the urinary collecting system. • Kidneys receive 25% of cardiac output • Sympathetic and parasympathetic nerve innervation • ADH and aldosterone • Collecting system of calyces, renal pelvis, ureters, and urethra
Functions of the Kidney: • Excretory functions: • removal of waste products from the body • regulation of fluids, electrolytes, blood pressure, and pH within the body • 3 processes: Filtration, Reabsorption, and Secretion
Non-Excretory or Metabolic functions: • Release of renin in response to renal ischemia to maintain normal BP • Production of prostaglandins • Production of erythropoietin • Vitamin D conversion to active form • Calcium and phosphorus regulation • Insulin degradation • Excretion of certain medications
Normal 24-hr urine output: • Kidneys filter about 180 liters of fluid/day! • GFR (Glomerular Filtration Rate): Normal GFR= 125 cc/minute • 99% of filtrate reabsorbed, 1% becomes urine (about 1 cc/minute) • Nomal24-hr urine output= 1440 or 1500 cc/day
What is Anasarca? • Generalized EDEMA due to Renal failure, glomerulonephritis, liver failure, Congestive heart failure, malnutrition. • Swelling is caused by effusion of fluid into the extracellular space.
What are the signs & symptoms of Anasarca? • Fluid retention • Shortness of breath • Massive edema • ++Mental functioning, irritability, tremors, ataxia or slurred speech. Nursing Interventions: • Monitor: vital signs, B/P, lung sounds (crackles), weight gain, I&O • Assess skin for color, presence of ecchymosis or rash, dryness and evidence of scratching, skin breakdown, decreased urine output
What is Azotemia • Azotemia refers to an unusually high amount of nitrogen waste products in the bloodstream (BUN). • Normally, the kidneys filter blood and expel waste in the form of urine. • Kidneys are unable to sufficiently remove urea, creatinine, and other nitrogen-containing compounds from the blood. • Symptoms: • Fatigue and confusion • Pruritus (itching) • HTN • Kidney failure without treatment (Emergency care)
What is Acute Renal Failure? (ARF) • Sudden inability of the kidneys to excrete nitrogenous waste products leads to azotemia. Three Types of Causes of ARF: • 1. Prerenal: caused by decreased renal blood flow Examples: thrombus in renal artery, hypovolemia due to hemorrhage • 2. Postrenal: caused by urinary obstruction Examples: Renal calculi (stones), tumors • 3. Intrarenal: Most frequent cause, damage to kidney itself Examples: primary renal diseases (acute pyelonephritis), systemic diseases (lupus), • ATN (acute tubular necrosis)= destruction of tubular epithelial cells caused by • trauma, infection, metabolic conditions, or NEPHROTOXINS
3 phases of ARF a) Oliguric Phase: <400 cc urine/day, lasts 8 to 14 days • Increased BUN, creatinine, K, low Na • Protein, red blood cells, and casts found in urine, low urine SG • Nausea, vomiting, lethargy, elevated BP • Need for short-term dialysis therapy • *The longer this phase lasts, the poorer the prognosis.
b) Diuretic Phase: kidneys begin recovery, lasts one week 1) Early diuretic phase: urine output >400 cc/day • Hypotonic urine (unable to concentrate urine, low SG) • Large amount of K and Na losses 2) Late diuretic phase: BUN returns to normal • Kidneys regain ability to concentrate
c) Recovery Phase: lasts 4 to 5 months, vulnerable to further renal insults Nursing Care: • Monitor renal function closely, teach pt to avoid potential renal insults (nephrotoxins) Leading Causes of Death in Acute Renal Failure: • 1) Hyperkalemia • 2) Infection
ARF (continue) • Pyelonephritis • Diabetes Melitus • Acute Tubular Necrosis • Benign Prostatic Hyperplasia (BPH) • Nephro/urolithiasis (renal stones) • Tumor • Urinary strictures • Injury Other: if not treated leads to: • Hyperkalemia, hypernatremia, • Hyperphosphatemia • HYPOCALCEMIA
What is Chronic Renal Failure? (CRF) • Irreversible loss of kidney function • Will require dialysis or transplant to replace the damaged kidneys • Also known as CKD or Renal Insufficiency • Causes of Chronic Renal Failure: • 1) Hypertension • 2) Diabetes • 3) Long history of analgesic abuse- Phenacetin • 4) Chronic urinary tract infections • 5) Glomerulonephritis • 6) Long history of renal stones • 7) Polycystic kidney disease • 8) Systemic Lupus Erythematosus (SLE)
Nursing Care • Same as for chronic renal failure, includes: fluid restriction, monitoring electrolytes • (hyperkalemia), management of mental status changes & GI complaints, patient/family education important
Clinical Manifestations of Renal Failure: I. Cardiovascular • 1) Anemia • 2) Pericarditis/ Pericardial Effusion • 3) Hypertension • 4) Congestive Heart Failure • 5) Hyperkalemia • 6) Edema II. Pulmonary • 1) Pulmonary Edema • 2) Dyspnea • 3) Pleural Effusion
III. Gastrointestinal • 1) Anorexia • 2) Nausea/Vomiting • 3) Diarrhea or Constipation • 4) Mucosal Ulcerations- GI Bleeding IV. Integumentary • 1) Pruritus • 2) Uremic Frost (rare) • 3) Easy Bruising
V. Neuromuscular/Behavioral • 1) Headache • 2) Daytime drowsiness/insomnia • 3) Confusion/ disorientation • 4) Asterixis (jerking movements of hands) • 5) Muscle weakness and cramping • 6) Peripheral Neuropathy • 7) Body image/ Self-Concept disturbances • VI. Endocrine/ Metabolic • 1) Calcium/Phosphorus Imbalance- Renal osteodystrophy • 2) Metabolic Acidosis
VII. Psychosocial • 1) Denial • 2) Depression/ Grief • 3) Dependency VIII. Sexual • 1) Impotence • 2) Amenorrhea • 3) Decreased sexual desire
Nursing interventions Fluid volume excess related to inability of kidneys to excrete fluid • Reinforce necessity of fluid and sodium restrictions in diet • Daily weights • Strict I & O • Assess for edema, SOB, increased respiratory rate, pulse, & BP, crackles in lungs • Check for JVD and pericardial friction rub
Riskfor injury: Fracture related to Ca-PO4 imbalances • Administer phosphate binders, calcium supplements, and Vitamin D as prescribed • Teach pt importance of taking these meds at home • *Phosphate binders need to be taken with meals • Monitor serum calcium & phosphorus levels • Assess for bone pain and limited mobility • Encourage activity and range of motion exercises as tolerated
Activity Intolerance related to anemia • Teach pt to plan activities to avoid fatigue with frequent rest periods • Monitor Hct and Hemoglobin levels • Administer iron supplements between meals and Epogen as prescribed
Altered nutrition: less than body requirements related to restricted diet, N/V, anorexia • Provide small frequent meals • Administer anti-emetics as ordered • Provide mouth care and hard candy or gum to improve taste • Monitor weight and labs (BUN, creatinine) to assess for effective dialysis
Sensory and perceptual alterations related to uremia • Assess mental status. Watch for confusion, irritability, behavioral changes, decreased attention. • Educate pt/family on relationship of uremia to mental status changes • Provide calm, non-stimulating environment • Provide short teaching sessions • Safety measures as appropriate • Reorient pt as necessary. Provide supportive environment.
Risk for infection related to uremic effects on immune system • Maintain aseptic technique for procedures • Assess for signs of infection (fever, chills, redness, edema, or drainage of site) • Instruct pt to avoid people with infections
Knowledge deficit related to lack of information about diet, meds, dialysis, self-monitoring • Teach pt/family about dietary restrictions and rationale for these. Dietary consult helpful. • Instruct pt/family about meds and administration times. • Provide information about dialysis treatment options, procedures, etc • Assess pt/family’s understanding of above and reinforce as necessary
Renal Medications • Multivitamin, Iron supplements (ferrous fumurate), Folic acid • Epogen- to prevent anemia • Tums (Calcium carbonate) or Basalgel- phosphate binders, can cause constipation • Shohl’ssolution- bicarbonate replacement, used for chronic metabolic acidosis • Rocalcitrol- Vitamin D supplement • Stool softeners • Sorbitol- artificial sweetener used as a laxative • Kayexalate- resin that binds K in GI tract, causes diarrhea
Warning • BEWARE OF MEDICATIONS that contain MAGNESIUM and PHOSPHORUS! • RF patients cannot excrete these substances. • Examples: Milk of Magnesia, Mylanta, Fleets Enema
Renal Nutrition • Typical renal diet: restricted protein, potassium, and sodium • Less restricted diet for Peritoneal Dialysis (PD) patients, lose protein through PD • Beware of salt substitutes, frequently contain KCl • Frequently require fluid restrictions - 1 liter/day • More liberal diet for PD patients.