Download
1 / 47
480 likes | 750 Views
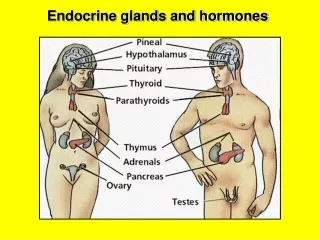
Pathology of Endocrine Glands - II. Thyroid. Endocrine Pancreas. Jaroslava Dušková Inst. Pathol. 1st Med. Fac. Charles Univ. Prague https://www1.lf1.cuni.cz/~jdusk/. Thyroid Gland History I. China (2nd mill.b.C.) description of goitre (Charvát 1935)

E N D
Pathology of Endocrine Glands - II Thyroid Endocrine Pancreas Jaroslava Dušková Inst. Pathol. 1st Med. Fac. Charles Univ. Prague https://www1.lf1.cuni.cz/~jdusk/
Thyroid Gland History I. • China (2nd mill.b.C.) description of goitre • (Charvát 1935) • Vitruvius (16.a.C.) goitre in the Alpine region • Warton (1656) „ Adenographia“ the term glandula thyreoidea • Luschka(1860) mechanical support of the laryngeal structures
Thyroid Gland History II. • Basedow (1840) hyperthyreosis • Köstl (1855 - Wien): • Der endemische Kretinismus als Gegenstand • der öffentlichen Fürsorge (habilit. thesis) • Gull(1873) hypothyreosis • Murray(1883) Therapy with bovinethyroid extracts
Thyroid Gland History III • Hashimoto (1912) struma lymphomatosa • Kendall (1914):Tyroxine discovery • Aron a Loebe(1929) TSHdiscovery • Adams a Purves(1952) LATS discovery
Thyroid Gland- embryology and fetal endocrinology • mouth epithelium, end of the 1st iu. month ductus thyreoglosus • lateral pharynx • ultimobranchial bodies C- cells. • parathyroid glands • fetal secretion starts at 12 weeks • effect on GROWTH • effect on DIFFERENTIATION
Thyroid Gland- anatomy • Weight in adults 15-20g • over60g(7g in a neonate)struma • lobus dexter • isthmus et lobus pyramidalis • lobus sinister • aberant, accesory, ectopic gland (polyclonality should help to tell from ca)
Thyroid Gland- physiology and regulations • hypothalamohypophysothyreoidal axis (TRH,TSH) • enzymes - deiodases • autoregulation influenced by iodine intake • immune system
Clinic scintigraphy SONOGRAPHY CT Pathology (biopsy) FNAB histology Morphological Thyroid Investigation
Main Tasks in the Thyroid Cytology • reduction of the unnecessary surgery • diagnosis of subclinical inflammation • EARLY DIAGNOSIS of NEOPLASMS
Thyroid Cytology - getting sample • needle 0.6-0.8mm • min. 2 punctions • aspiration • nonaspiration • cyst: evacuate and aspirate with the second punction the periphery • fluid: whole volume for cytology
Fixation air dried etanol / spray (cytospin) CYTOBLOCK Staining: MGG HE polychrom all histo. imunocyto TGB,calcitonin, parathormon Thyroid Cytology- processing
Regressive changes of thyroid gland • dystrophy: amyloid deposits, calcification • atrophy: due to the lack of TSH stimmulation, postinflammatory • necrosis: only in hyperplastic or neoplastic goitre
Thyreoiditis • NON-SPECIFIC • purulent • non-specific granulomatose de Quervain • lymphocytic (Hashimoto) • hypertrophic • atrofic • focal • invasive sclerosing Riedel • SPECIFIC • tbc • syfilis • sarcoidosis
Non-Specific Granulomatose Thyreoiditis de Quervain (1904) • Synonyma: „Giant cell“ • „Subacute non-purulent“ • Clin.features: Oedema, pain, eufunction, may be also silent • Histol. features: dispersegranulomas • with giant cells • Course: spontaneous healing by 2-4 weeks
Thyreoiditis lymphoplasmocellularis Hashimoto - HTHashimoto, H.: • Zur Kenntniss der lymphomatösen Veränderung der Schilddrüse • (struma lymphomatosa) • Arch.f. klin. Chir. 97, 1912, 219
Original HT Description • Macro - diff. parenchymatose goitre firm, elastic, gray-yellow Micro - diffuse lymfoplasmocellular lymph. folicules ONCOCYTES
Etiopathogenesis of HT • Etiology:unclear - viri ? • Pathogenesis: • dysregulation of T lymphocytes • IL-1 expression Fas molecules on the surface of thyreocytes (they have FasL) apoptosis activation • Activity: CD 44 proteoglycan influencing migration and lymphocyte proliferation, and metastasizing
Course of HT a) progressive • oncocytic transformation loss of thyreocytes, • transformation to a lymph- node-with-ca- meta image • hyperfunction folowed by hypofunction
Course of HT b) regressive • loss of parenchyma, • fibrosis • hypofunction
Course of HT c) neoplasia • carcinoma • lymphoma (mostly B - MALT)
Thyroid Malignant Lymphomas • 2% thyroid primary malignancies • mostly women with HT • clinically rapid growth, often hypothyreosis • mostly B (MALT), features of lymphoepithelial lesion • both LG and HG • diff. dg. HT • clinical and cytology suspicion • dg. excision
Chronic Sclerosing Thyreoiditis Riedel (1910) • Synonyma:„Invasive Fibrotising“ „ Iron hard (eisenharte) goitre“ • Clin.features: • slight assym. edema • fixation to surrounding structures • eu- or hypofunction • tracheal stenosis • recurrens paresis • Histol. features: • tissue destruction • fibrotisation • fixation to surrounding structures • involment of the neck vessels • Course: Stabilisation, possible progression
Thyreoidal Syndromes • hypothyreosis • inborn – cretinism • endemic, sporadic • acquired – myxedema • hyperthyreosis - thyreotoxicosis
Hypothyreosis CRETINISMUS • disturbances of growth & differentiation BRAIN LUNG BONE
Acquired Hypothyreosis - MYXEDEMA • decreased metabolism • bradycardia, low blood pressure, water retention, obstipation • intolerance of cold • lowered lipolysis • weight increase • hyperlipemia ATHEROSCLEROSIS
Thyreoidal Syndromes • hypothyreosis • inborn – cretinism • endemic, sporadic • acquired – myxedema • hyperthyreosis - thyreotoxicosis
Hyperthyreosis • increased metabolism • tachycardia, high blood pressure, fibrilation, • hypercalciuria, diarrhoe • intolerance of warm • increased lipolysis, glycogenolysis • weight decrease • hyperglycemia, diabetes • muscle weekness, insomnia, exophtalmus, pretibial myxedema
Processing of Thyroid Resecate • orientation • division • lobus dx. • isthmus (+lobus pyramidalis) • lobus sin. • cutting in cca 3mm thick lamellae • revision and extensive/complete blocking of the encapsulated nodules periphery • any suspicious focus for histology
Histological diagnosis microfollicular adenoma follicular carcinoma Cytological features highly cellular smears few colloid microfollicular formations thyreocytes regular, small or slightly enlarged bare nuclei regressive changes: mostly absent Folicular Neoplasia (proliferating microfollicular lesion)
Oncocytic Tumours • adenoma • architecture follicular, trabecular • cellular atypiae without predictive value for biological behaviour • more risk in case of solid architecture • EXCLUDE • ANGIOINVASION, CAPSULOINVASION
Oncocytic Tumours • carcinoma • oncopapillary (may lack ground glass nuclei !) • oncofollicular • must exhibit • ANGIOINVASION and/or • CAPSULOINVASION (all capsule thickness with extracapsular expansion)
Histological variants - WHO microcarcinoma encapsulated follicular diff. sclerosing oxyphil cell Histological variants additional tall cell columnar cell macrofollicular with desmopl.stroma hyal. trabecular ca Papillary Carcinoma
Cytologicalfeatures general highly cellular smears few colloid waxy colloid, may be absent architecture phragments of papillae groups trabecular microfollicular syncytial formations squamous metaplasia psammomata NUCLEI enlarged non - circular overlapping grooves pseudoinclusions Papillary Carcinoma
origin fom C-cells clinical forms : (parafollicular) sporadic familiar MEN 2a MEN 2b Medullary Carcinoma
MEN 2a medullary ca parathyr. adenoma pheochromocytoma MEN 2b MEDULLARY CA marphanoid habitus mucous neuromas pheochromocytoma parathyr. adenoma - Medullary Carcinoma familiar forms
Medullary carcinoma • C-cells(parafollicular) • sporadic • familiar • MEN 2a • MEN 2b
Histological diagnosis Calcitonin + amyloid +- argyrophilia + Medullary carcinoma
Histological diagnosis architecture may mimic any other thyroid ca!!! (WHO) Calcitonine + amyloid +- argyrophilia + Medullary Carcinoma
Cytological types large cell small cell fusocellular plasmocytoid Medullary Carcinoma
highly malignant neoplasm of the old age with rapid progression origin: non diagnosed differentiated ca hyperplastic goitre chronic inflammation without preceeding goitre Undifferentiated Carcinoma(anaplastic)
Undifferentiated Carcinoma • Histological variants(often combined) • fusocellular • small cell (?)exclude lymphoma! • giant cell (monstrous cells) • squamous metaplasia • composed • lmsa, rmsa,osa, chsa, hae, MFH, classify as carcinoma!
Other Types of PrimaryThyroid Carcinomas • epidermoid • mucoepidermoid • mixed follicular and mucoepidermoid
Metastases into Thyroid • kidney • lung • breast • other
Islets of Langerhans (1869) • adults 100 000 -1000 000 • cell types: B - insulin A - glucagon D – somatostatin PP – pancreatic polypeptide D – vasoactive intestinal polypeptide
Islets of Langerhans - regressive changes • fibrosis (postinflamm.) - DM I • mucoviscidosis – DM 10x frequency • hyalinosis, amyloidosis
Islets of Langerhans - progressive changes • hyperplasia –diabetic embryopathy • nesidioblastosis - tumours • nesidioma ( event. in MEN I) • (insulinoma, glucagonoma, somatostatinoma,VIPoma, PP-oma, G cells -gastrinoma, EC – serotonin - carcinoid • neuroendocrine carcinoma
Islets of Langerhans - syndromes • hyperfunction • hypoglycemia (weekness , sweating, tremor, coma) • Zollinger-Ellison, Werner Morrison, glucagonoma • hypofunction – insulin hyperglycemia • acute : polydipsia, ketoacidosis, coma, liver steatosis , brain edema • chronic: diabetes mellitus: microangiopathy, macroangiopathy, neuropathy, retinopathy,embryopathy