Download
1 / 29
290 likes | 347 Views
Learn about pain perception, transmission, opioid agonists, antagonists, and management of pain with CNS analgesic drugs. Explore the impact of neurotransmitters and pain classification on medication effectiveness.

E N D
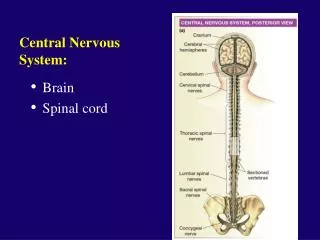
Central Nervous System Analgesic Drugs – Lilley – Ch 11 CNS Depressants & Muscle Relaxants – Lilley– Ch 13 CNS Stimulants -Lilley – Ch 14 Antiepleptic Drugs – Lilley – Ch 15 Antiparkinsonian Drugs – Lilley -- Ch 16
CNS Pharmacology Objectives • Discuss the the actions and uses of an opioid agonist, agonist-antagonist, and antagonist • Describe how the nursing process is applied to clients receiving sedative-hypnotic agents • Describe the role of the nurse in promoting client compliance with drug therapy for seizure activity • Identify the variety of conditions and disorders being treated with CNS stimulants • Describe the actions and intended effects of the classes of medications used in the treatment of Parkinson’s disease
CNS- Analgesic AgentsPain • Defn: • Medications that relieve pain without causing loss of consciousness • Painkillers
CNS – Analgesic AgentsPain • Pain • Whatever the patient says it is – Perception • It exists whenever the patient says it exists • It’s an unpleasant sensory and emotional experience associated with actual or potential tissue damage • Pain is a personal and individual experience
CNS– Analgesic AgentsPain • Subjective: • Pain Threshold: • The level of stimulus needed to produce the perception of pain • A measure of the physiologic response of the nervous system • Pain Tolerance: • The amount of pain a patient can endure without its with normal function with normal function • The point at which the pain becomes unbearable
CNS – Analgesic AgentsClassification of Pain • Classification of pain by onset and duration: • Acute pain: • Sudden onset • Usually subsides once treated • Chronic pain: • Persistent or recurring • Often difficult to treat
CNS – Analgesic AgentsClassification of Pain • Classification of Pain • Somatic • Visceral • Vascular • Referred • Neuropathic • Phantom • Cancer • Psychogenic • Central
CNS – Analgesic AgentsPain Transmission • Pain Transmission – Gate Theory • Impulses travel from damaged tissues and are sensed in the brain • Many current pain theories are aimed at altering this system • Substances released that stimulate nerve endings: • Bradykinin, histamine, potassium, prostaglandins, serotonin • Nerves stimulated: • “A” fibers: large fibers covered with myelin sheath, with rapid conduction – results: sharp & well localized pain • “C” fibers: small fibers with no myelin sheath, with slow conduction – results: dull and non-localized pain
CNS – Analgesic AgentsPain Transmission • Pain fibers enter the spinal cord and travel up to the brain • Enter through the dorsal horn – “the gate” • The gate regulates the flow of sensory impulses to the brain • If no impulses are transmitted to higher centers in the brain, there is no pain perception • Activation of “A” fibers - closes the gate • Allows the brain to evaluate, identify and localize the pain & control the gate before it is open • Activation of “C” fibers – opens the gate
CNS – Analgesic AgentsPain Transmission • Body has endogenous neurotransmitters • Enkephalins • Endorphins • Produced by body to fight pain • Bind opioid receptors & inhibit transmission by “closing the gate” • Examples: • Runner’s high • Rubbing a painful area stimulates large sensory fibers – result: gait closed, pain recognition reduced • Opiates use the same pathway
CNS – Analgesic AgentsAgonist • Binds to an opioid pain receptor in the brain and causes an analgesic response
CNS – Analgesic AgentsOpioidAnalgesics • Opioid pain relievers: Narcotics that contain “opium”, derived from the opium poppy • Very powerful • Addictive • Indications: PAIN Management • alleviate severe to moderate pain • Often given with adjuvant analgesic agents to assist pain relief: NSAIDS, Antidepressants, Anticonvulsants, corticosteroids • Cough center suppression • Treatment of diarrhea • Balanced anesthesia
CNS –Analgesic AgentsAntagonists • Reverse the effects of these agents on pain receptors • Bind to a pain receptor and exert no response • Also known as competitive antagonists • Medications: • naloxone (Narcan) – treat overdose • Naltrexone (Trexan) – maintenance of opioid-free state & psychosocial tx of alcoholism
CNS – Analgesic AgentsSide Effects • Euphoria • CNS depression • Nausea and vomiting • Respiratory depression • Urinary retention • Diaphoresis and flushing • Pupil constriction (miosis) • Constipation • Itching
CNS – Analgesic AgentsOpioid Overdose Triad • Respiratory depression • Respiratory rate <12/min, dyspnea, diminished breath sounds, or shallow breathing • Decreased level of consciousness • Pinpoint Pupils (miosis)
CNS – Analgesic AgentsOpioid Effects • Tolerance • Common physiologic effect of chronic opioid tx • Larger doses are required to produce the same level of analgesia • Physical Dependence • Physiologic adaptation of the body to the presence of an opioid Tolerance and physical dependence are expected with long term opioid treatment, and should not be confused with: • Psychological Dependence • Pattern of compulsive drug use characterized by continued craving for an opioid and the need to use the opioid for effects other than pain relief
CNS – Analgesic AgentsWithdrawal / Abstinence • Syndrome • Occurs when abruptly discontinued or when an opioid antagonist is administered • anxiety, irritability, chills & hot flashes, joint pain, lacrimation, rhinorrhea, diaphoresis, nausea, vomiting, abdominal cramps, diarrhea
CNS – Analgesic AgentsNon-opioids • acetaminophen (Tylenol): blocks peripheral pain impulses by inhibition of prostaglandin synthesis & lowers febrile body temp – hypothalamus • Max dose for healthy adult 4,000 mg per day • Check combinations of drug products • acetylsalicylic acid (Aspirin): anti-inflammatory, anti-pyretic, analgesic, anti-rheumatic properties • Check when ordered with NSAIDs or Plavix
CNS -- Analgesic AgentsNon-steroidal anti-inflammatory drugs • NSAIDs – reduce inflammation • Block Leukotriene (lipoxygenase) pathway • Salicylates • Cox1 isoform of the enzyme promotes synthesis of homeostatic prostaglandins • Indomethacin (Indocin); ibupofen (Motrin); naproxen (Naprosyn); nabumetone (Relafen) • Cox2 inhibitors block the cyclooxygenase cox2 pathway - prevent GI side effects • Celecoxib (Celebrex)
CNS – Analgesic AgentsMedication Orders • Joint Commission Requirements • Pain medication for severe, moderate, and/or mild pain Example: Morphine 5 mg IM q4h prn severe pain Percocet 1-11 tablets q6h prn moderate pain Tylenol 650 mg po q4h prn mild pain
CNS – Analgesic AgentsInteractions • Dangerous interactions may occur if taken with alcohol • Should not be taken in the presence of: • Liver dysfunction • Possible liver failure • When taking other hepatotoxic drugs
CNS – Analgesic AgentsNursing Implications • Assessment • Allergy History / Idiosyncratic Reactions • History of alcohol use • Medical history – possible contraindications • Medication reconciliation – possible drug interactions • Thorough pain assessment – Fifth Vital Sign • Intensity, character, onset, location, description, precipitating and relieving factors, type, remedies, and other pain treatments • Pain Scale / Nonverbal • Baseline vital signs and pulse oximetry • Monitor for side effects, change in pt status, & status of pain relief
CNS – Analgesic AgentsNursing Implications • Patient Education • Do not take other medications or OTC medications unless prescribed by physician • Pain scale • Signs & Symptoms of drug allergies or adverse effects • Safety measures • Pain management – includes both pharmacologic and non-pharmacologic approaches: • Position of comfort, distraction, therapeutic touch, comfort foods & beverages, visitors, spirituality, presence!
CNS – Analgesic AgentsNursing Implications • Nursing Actions: • Administer oral forms with food to minimize gastric upset • Ensure safety measures – prevent orthostatic hypotension • Withhold dose and contact physician with any change in pt status • Check dosages carefully • Follow proper administration guidelines – po, sq, IM, IV – including dilution, rate of administration • Side Effects: constipation – increase fluids, stool softeners
CNS – Analgesic AgentsNursing Implications • Monitor for therapeutic effects • Decreased complaint of pain • Decreased severity of pain • Increased periods of comfort • Improved activities of daily living, appetite, and sense of well-being • Decreased fever (acetaminophen & NSAIDs)
CNS – Analgesic Agents • For the best results in treating severe pain associated with pathologic spinal fractures related to metastatic bone cancer, which type of dosage schedule should be used? Plan medication administered: • a. As needed. • b. Around the clock. • c. On schedule during waking hours only. • d. Around the clock, with added doses as needed for breakthrough pain.
CNS Analgesic Agents • A patient is receiving an opioid via a PCA pump as part of the postoperative pain management program. During rounds, the nurse notices that his respirations are 8 breaths per minute and he is extremely lethargic. After stopping the opioid infusion, what should the nurse do next? • a. notify the charge nurse • b. administer oxygen • c. administer an opiate antagonist per standing orders • d. perform a thorough assessment, including mental status examination