Download
1 / 39
390 likes | 533 Views
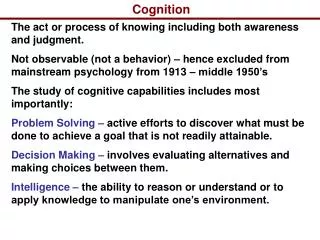
Cognition. Aphasia - a disturbance of language use. Because of brain pathology, the patient becomes unable to use words as symbols.

E N D
Cognition • Aphasia- a disturbance of language use. Because of brain pathology, the patient becomes unable to use words as symbols. • Amnesia- a loss of memory, It can be retrograde (loss of memory for events that occurred before a certain time) or anterograde (loss of ability to form new memories) • Apraxia- the inability to perform a motor behavior, even though the muscles and nerves required for the motion are themselves intact. • Agnosia- the inability to recognize familiar objects, even though the senses required for this recognition are intact • Loss of executive functioning- difficulty planning , organizing, sequencing, or abstracting information • Prosody- • Confusion- inexact term used to describe slowed thinking, loss of memory, or disorientation. • Functional- term used to describe d/o’s for which they can no find no basis in brain anatomy, chemistry, or physiology.
Case Example • 42 school principal with recent history of having sexual relationships with several of her students • No previous history of sexual assault, but was sexually abused as a child • Possible diagnoses?
Delirium • Rapidly developing, fluctuating state of reduced awareness in which the following are true: • trouble shifting/focusing attention, and • at least one defect of memory, orientation, perception, or language and • symptoms are not better explained by a dementia • Causes- GMC, Substance-Induced, Multiple Etiologies*, and NOS
Dementias(how differs from Delirium) • Memory loss as well as other cognitive deficits (e.g... amnesia, aphasia, apraxia, agnosia, and loss of executive functioning) • No prominent impairment in the ability to focus or shift attention • Cause can usually be found within the CNS instead of elsewhere in the body. • Dementia is relatively fixed and unchanging • Recovery is not common • Types- DAT, Vascular, GMC, Substance-Induced, Multiple Etiologies, NOS
Assessment Issues • MMSE (page 71 Spreen & Strauss) • Most dementia studies have < 21 as a cuttoff • Imaging • http://www.med.harvard.edu/AANLIB/home.html
DAT Facts • Cost is over 100 billion dollars annually in the United States • Average age at diagnosis is 80 • 1-2% @ age 65 • 1-5% @ age 80 • 50% “have Sx” @ 90 • Heritibility rate is 40% in those with early onset dementia in sibs and parents
Lewy Body Disease/Dementia • Protein deposits found on deteriorated nerve cells throughout the brain • Fluctuations in cognition, with confusion and hallucinations in early stages • Autopsies show Lewy bodies in cortex without tangles seen in DAT • Genetic changes seem to trigger neurodegenerative process • Worse visuospatial functioning and better memory functioning compared to DAT
Beh. Problems of Dementia • Agitation/Aggression • Sundowning • ADL decrements • Combativeness • Psychosis • Disinhibition • Incontinence
Agitation/Aggression in Dementia • Most common psychiatric referral (40-80%) • Negative correlation with cortical serotonin levels • More common in mid to late stages • Responds to a variety of pharmacotherapy
Afternoon Sundowning in Dementia • Possibly due to fatiguability • Increase cognitive cues and structure late in day • Nap after lunch • Dose of psychotropics around 3PM
Nocturnal Sundowning in Dementia • Few orienting cues at night coupled with tendency toward nocturnal awakening • Increase phototherapy or daylight • Sleep hygiene (no naps or caffeine) • Hypnotics (e.g. Chloral hydrate, Trazadone) • Don’t forget the nightlight
Combativeness in Dementia • Common in pts. with executive dysfunction • Intervention: limit goals; negotiate, don’t drill!; pre-medication with lorazepam • Visual agnosia may lead to fearfulness in severely demented patients. (go slow/easy) • Usually able to read emotional prosody better than comprehend words
Psychosis in Dementia • 50% Prevalence • Usually doesn’t cause problems • May predict more rapid progression • Treatments include reality therapy (drive around the house/block) and a host of neuroleptics
Disinhibition in Dementia • No goal oriented behavior, therefore very responsive to impulses • Consider beta-blockers and Progesterone • Wandering (Rx.: activity for stimulation seekers or decrease neuroleptics) • Screaming • in late stages • rule out pain • increase stimulation
Incontinence and Dementia • Common in strokes and late stage DAT • Depends • Often the most difficult symptom for caregivers to cope with
Depression and Dementia • 20 to 30% prevalence, mostly early • Most important treatable cause of diminished quality of life • Predictors include past history or family history of depression • Differential: Depressed patients demonstrate cognitive response to antideps. • Depression secondary to Dementia • Client and Cargiver
Management Issues in Dementia • Feedback • Family meeting and long-term planning • When is it time? (driving, tell dx, safety-proof house, support group, ALF/ECF) • Education (e.g. groups, bibliotherapy) • Interacting with patient • Caregiver burden*
Implications of dementia • Driving • POA • Competency to make decisions • Need for re-evaluation
Competency to Stand Trial • 1. Capacity to appreciate charges or allegations • 2. Capacity to appreciate the range and nature of possible penalties which may be imposed • 3. Capacity to understand the adversary nature of the legal process • 4. Capacity to disclose to attorney facts pertinent to the proceedings • 5. Capacity to manifest appropriate courtroom behavior • 6. Capacity to testify relevantly
Amnestic Disorders • No requirement for reduced ability to focus or shift attention • Memory is affected far more than any other function, sometimes to the extent that pts. will forget conversations that took place only a few minutes earlier. • Confabulation (trying to hide a loss of memory by making up experiences to fill information void) is common early in the course of illness. Most common in early phases. • Types- GMC, Substance-Induced, or NOS
Other Causes of Cognitive Symptoms • Age-Related Cognitive Decline • Dissociative Disorders • Pseudodementia • Malingering • Factiscious Disorder with Predominantly Psychological Signs and Symptoms
The Neuropsychological Impact of Concussion in College Football:A Multi-center Analysis of Mild Traumatic Brain Injury(JAMA, 1999)Michael W. Collins, Ph.D.Duane E. Dede, Ph.D., et al. • Participating Universities: • Michigan State University • University of Florida • University of Pittsburgh • University of Utah • Sources of Funding: • Arthur J. Rooney Foundation • Blue Cross/Blue Shield of MI • Michigan State U. Foundation • U. of Florida Golden Opportunity Fund
Co-Investigators and Collaborators • Sam Sears, Ph.D.; Benjamin Phalin, B.S.; Dave Moser, PhD.; Guido Urizar, B.A., Chris Houck, B.A., Arthur Day, M.D.; Peter Indelicato, M.D.; Guy Nicholette, M.D.; Mike Wasik, A.T.C., M..Ed; Matt Walser, A.T.C.; Chris Patrick, A.T.C., M.A.; Tom Kaminski, Ph. D. Mary-Beth Horodyski, Ed.D. • David Cordry, M.A.; Michelle Klotz Daughtery, M.A.; Mark Lovell, Ph.D.; Jeffrey Covan, D.O.; Randy Pearson, M.D.; Sally Nogle, A.T.C., M.A.; Jeff Monroe, A.T.C., M.S. • Scott Grindel, M.D.; Douglas McKeag, M.D.; Kevin Connelly, A.T.C., M.A.; Rob Blanc, A.T.C., M.A.
Project Timeline Day 5 24 hours Concussion Baseline: Preseason testing Post season testing Day 3 Day 7
Grade 1 ConcussionHopkins Delay Total Score (Standard Score) (Mean =100; SD =15)))
Key Findings • LD & previous concussion history were more significant than concussion grade • More prevalent than previously reported • Demonstrate “recovery curve” • Empirical findings will offer a more informed basis for guidelines • Memory testing is particularly sensitive
Retired athletes • Cognitive and emotional impairments reported in FB, soccer & boxing • Significant orthopedic comorbitiy • Players Association • UNC-CH Center for Professional Athlete Rehabilitation
Second Impact Syndrome(SIS) • Individuals with two blows to the head within a short time frame are at sudden risk of sudden, irreversible and fatal diffuse cerebral swelling with delayed catastrophic deterioration • From 1992-1995, there have been 17 documented fatalities in males involved in sports (boxing, skiing, ice hockey and football). • All football SIS deaths were in HS students • Fatal in 50% of cases
Case Study 20 yo EA defenseperson 4 Grade 2 concussions 1995-Head to head (2 days of Sx.) 1996-Head to head (2 days of Sx.) 1998-Ball to RTL (30 days of Sx.) 1999-Ball to RTL(40 days of Sx.) All EEGs and MRIs negative 1999 testing c/o mild headache and irritability SDMT Memory (-1.9 SD) Pegsdom (+1.5 SD)
Children and SRC • Limit heading • Proper technique • Protective devices • Follow return to play guidelines after initial concussion • Serial NP testing • Repeat CT scan
Protective Headgear? • Ziejewski (2002) reported decreased incidence and severity • Face masks were associated with less severe symptoms • Compliance poor in male athletes, especially rugby
Other impact of SRC • Emotional regulation • Controversies in testing • Definition of SRC • IMPACT vs. other modes • Frequency of testing • Return to play issues • Individual differences